|
Back to Annual Symposium Program
Increased Hospital Use of Carotid Artery Stenting (CAS) Over Carotid Endarterectomy (CEA) is Associated With Inferior Outcomes in Asymptomatic Patients
Theodore H. Yuo, MD, Howard Degenholtz, PhD, Rabih A. Chaer, MD, Kevin L. Kraemer, MD, Michel S. Makaroun, MD.
University of Pittsburgh, Pittsburgh, PA, USA.
OBJECTIVES: CAS has been shown to have higher perioperative stroke and death (PSD) rates than CEA in symptomatic, but less convincingly in asymptomatic patients. Limited CAS experience has been blamed for worse outcomes. We sought to compare the PSD rate of CAS versus CEA in an administrative database to determine if CAS usage variation is linked to PSD in asymptomatic patients at the hospital level.
METHODS: Using California hospital discharge data from 2005 through 2009, we identified CAS and CEA procedures and hospitals where they were performed. Preoperative symptom status was determined using ICD-9 and administrative codes. Propensity scores based on comorbidities and demographics were generated to identify a matched and balanced cohort of CEA and CAS patients. We used logistic regression to identify risk factors for PSD, calculated CAS rates as a proportion of all carotid revascularization (CR) procedures for each hospital, stratified hospitals into groups based on the proportion of CR that was CAS, and performed non-parametric test for trend to compare PSD rates.
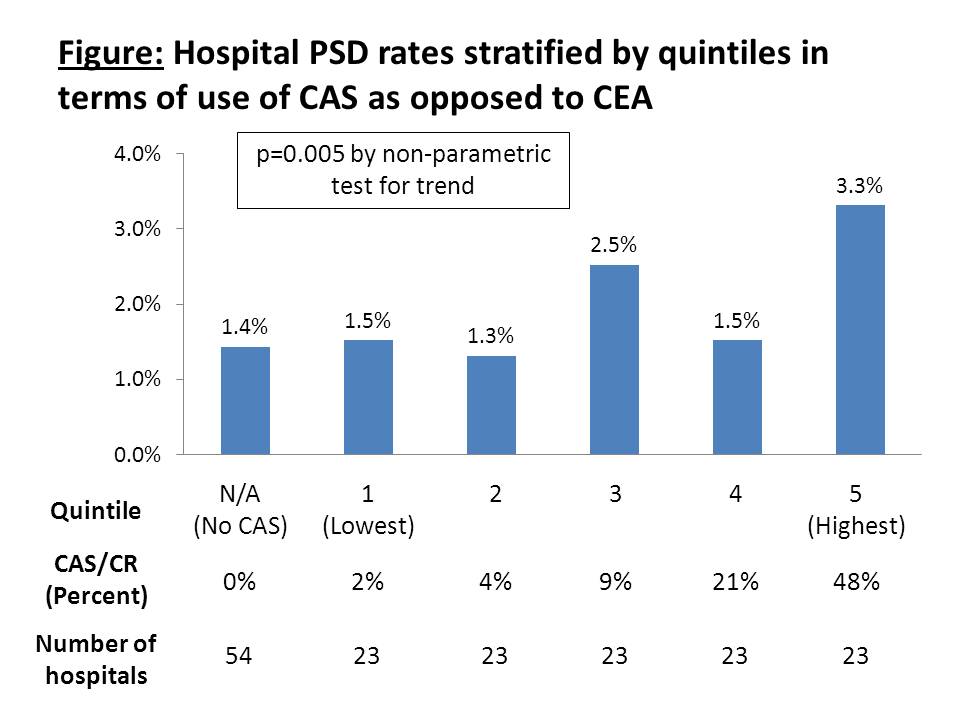
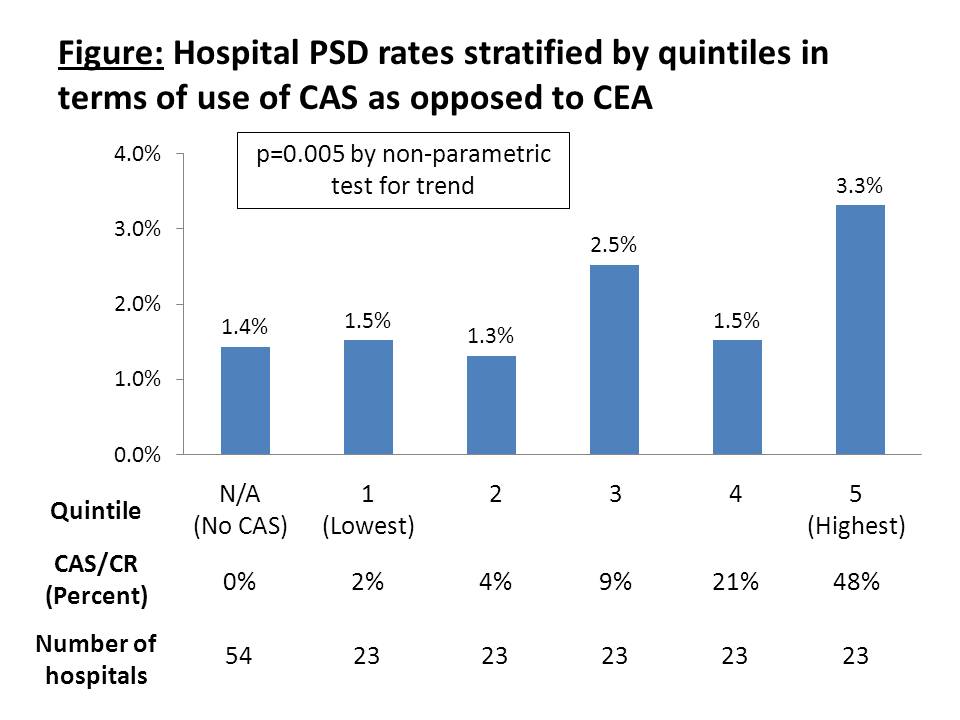
RESULTS: From 2005 to 2009, 3,549 CAS and 26,792 CEA were identified that treated asymptomatic patients in 270 hospitals. PSD occurred in 133 CAS and 446 CEA patients, yielding unadjusted PSD rates of 3.7% and 1.7%, respectively (p<0.001). Compared with CAS patients, CEA patients were more likely to be older than 70 (67% vs. 64%, p<0.001), but less likely to have 3 or more comorbidities (37% vs. 40%, p<0.001). After propensity score matching and eliminating hospitals with fewer than 20 CR over 5 years, 18,297 patients in 169 hospitals were available for analysis. Logistic regression demonstrates CAS is significantly associated with increased PSD risk (OR 2.497, p<0.001). Patients undergoing CR in hospitals that perform CAS more frequently, in terms of CAS as a proportion of CR, had higher PSD rates than patients in hospitals that performed CAS less (Figure).
CONCLUSIONS: CEA has a lower PSD rate compared to CAS in asymptomatic patients. PSD rates were elevated in hospitals with higher proportions of CAS as a proportion of CR, suggesting that increased use of CAS in a hospital is associated with worse patient outcomes.
Back to Annual Symposium Program

|