|
Back to Annual Symposium Program
Natural History of Saccular Aortic Aneurysms
Eric K. Shang, M.D., Derek P. Nathan, M.D., William W. Boonn, M.D., Ivan A. Lys-Dobradin, Ronald M. Fairman, M.D., Edward Y. Woo, M.D., Grace J. Wang, M.D., Benjamin M. Jackson, M.D..
University of Pennsylvania, Philadelphia, PA, USA.
Objectives: Repair of saccular aortic aneurysms (SAA) is frequently recommended based on a perceived predisposition to rupture, despite little evidence that these aneurysms have a more malignant natural history than fusiform aortic aneurysms.
Methods: The radiology database at a single university hospital was searched for the computed tomographic (CT) diagnosis of SAA between 2003 and 2011. Patient characteristics and clinical course, including the need for surgical intervention, were recorded. SAA evolution was assessed by follow-up CT, where available. Multivariate analysis was used to examine potential predictors of aneurysm growth rate.
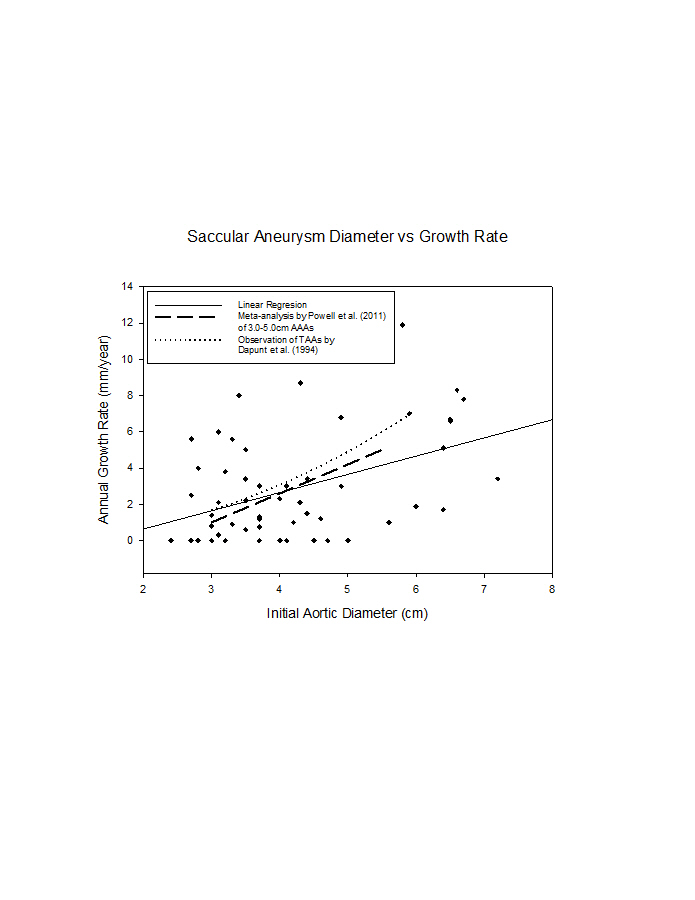
Results: 322 saccular aortic aneurysms were identified in 284 patients. There were 153 (59.0%) men and 131 women with a mean age of 73.5 ± 10.0 years. SAA were located in the ascending aorta in 2 (0.6%) cases, the aortic arch in 24 (7.4%), the descending thoracic aorta in 227 (70.5%), and the abdominal aorta in 79 (24.5%). 113 (40.0%) patients underwent surgical repair of SAA. 63 patients (54.3%) underwent TEVAR, 24 underwent EVAR (20.7%) and 29 (25.0%) required open surgery. The average maximum diameter, measured perpendicular to the aortic lumen centerline and including the aortic lumen diameter, of SAA was 5.0 ± 1.7 cm. In repaired aneurysms, the mean diameter was 5.4 ± 1.4 cm; in unrepaired aneurysms it was 4.4 ± 1.1 cm (P<0.001). Eleven patients (3.9%) had ruptured SAA on initial scan. Of the initial 284 patients, 50 patients (with 54 SAA) had CT follow-up after at least 3 months (mean 23.2 ± 19.0 months). Aneurysms grew on average 2.8 ± 2.9 mm/year. Aneurysm growth was only weakly related to initial aortic diameter (R2 = 0.19 by linear regression, P = 0.09 by multivariate regression). Decreased calcium burden (P = 0.03) and increased patient age (P = 0.05) predicted increased aneurysm growth.
Conclusions: SAA were not found to have a markedly malignant natural history. Close clinical follow up in the individual patient and further clinical research are necessary to determine the optimal management of SAA. 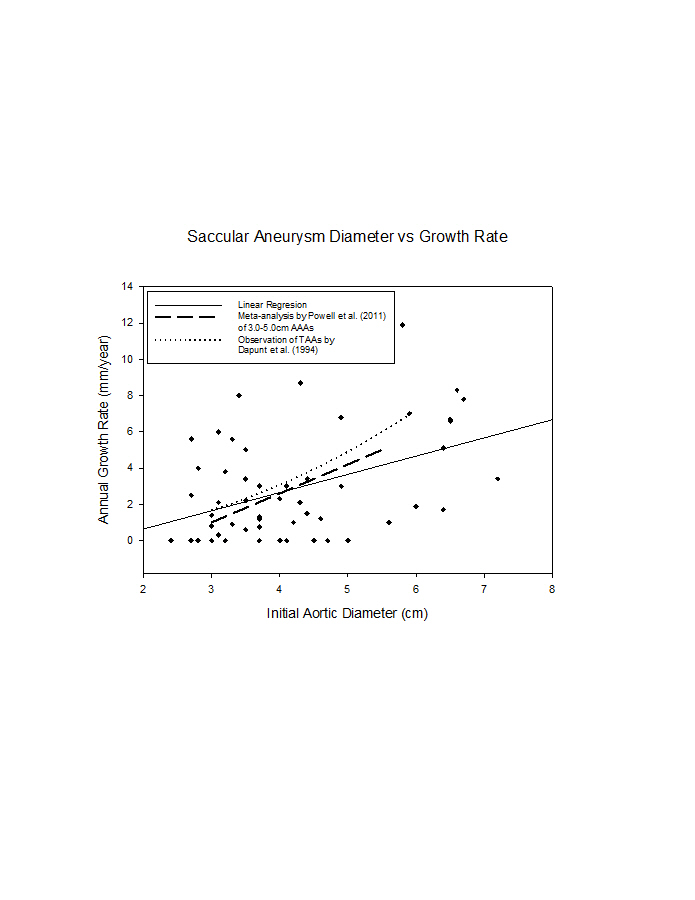
Back to Annual Symposium Program

|