|
Back to Annual Symposium Program
Endoconduits to facilitate endovascular repair of aortic aneurysms in high-risk patients with difficult iliac access
Tiziano Tallarita, MD, Gustavo S. Oderich, MD, Alexandre A. Pereira, MD.
Mayo Clinic, Rochester, MN, USA.
Purpose: This study describes the technique and outcomes of endovascular conduits to facilitate endovascular aortic aneurysm repair in patients with difficult iliac access.
Methods: We reviewed the clinical data of all consecutive patients treated by endovascular aortic aneurysm repair using endovascular conduits (2006-2010). Endoconduits were indicated in high-risk patients with small or occluded iliac arteries. Inadvertent hypogastric artery occlusion was avoided in patients with thoracic or thoracoabdominal aneurysms (TAAA) to minimize risk of spinal cord injury. The endoconduit technique consisted of controlled iliac artery disruption using >9mm self-expandable stent grafts (Figure 1) or angioplasty and stenting for recanalization of larger iliac arteries. End-points were technical success, morbidity, mortality, patency and freedom from re-interventions
Results: There were 11 patients, 10 male and 1 female, with mean age of 74±8 years. Aneurysm extent was infrarenal in 7 patients, pararenal in 3 (Figure 2) and TAAA in 1. The inner iliac artery diameter averaged 5±2 mm. The endoconduit included the external iliac artery in all patients, and extended into the common iliac artery in 7. A patent hypogastric artery was sacrificed in 4 patients. The average stent diameter and length was 11±1 and 84±24 mm, respectively. Technical success was achieved in all cases, allowing introduction of 20 to 24 Fr sheaths. Endovascular repair required infrarenal bifurcated stent grafts in 7 patients and fenestrated endografts in 4. There were no operative deaths. Four patients had postoperative complications including respiratory failure, minor stroke, renal insufficiency and iliac limb kink in one patient each. There were no pelvic ischemic complications, spinal cord injuries or uncontrolled arterial disruptions. After a median follow up of 28 months, all endoconduits remained patent. One patient required muscle flap coverage for late groin wound infection.
Conclusion: Endovascular conduits are useful to facilitate endovascular aortic aneurysm repair in patients with difficult iliac access because of small size or occluded iliac arteries. The technique is safe, effective and has excellent patency. 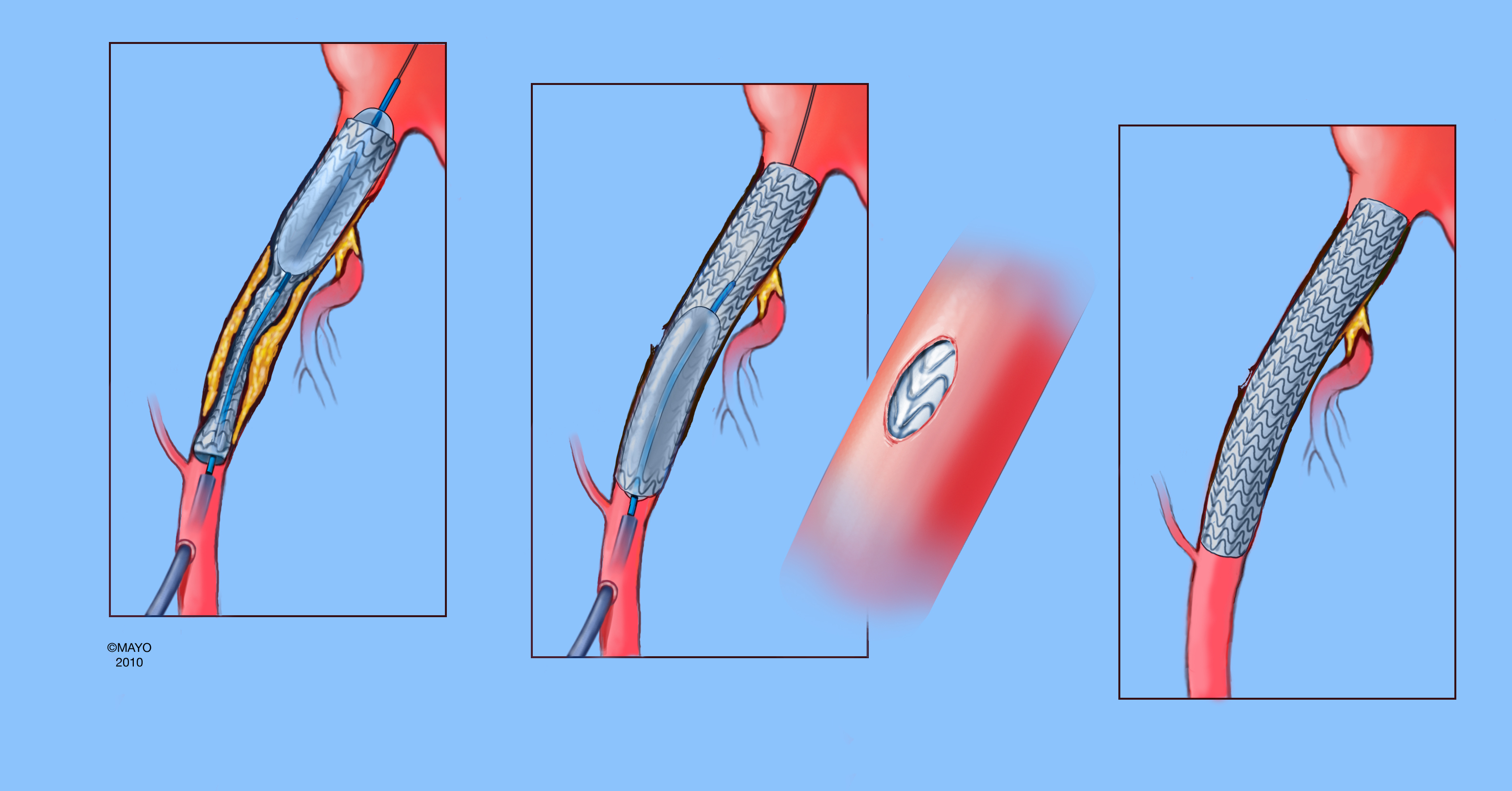 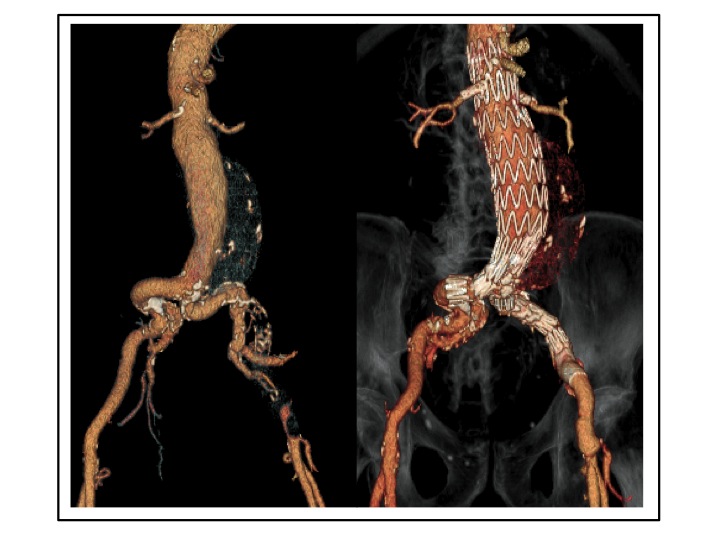
Back to Annual Symposium Program

|


