|
|
 |
Back to Annual Symposium Program
Illustration of Workflow with Results of Fourteen Cases Employing Angio CT and Fluoroscopic Needle Guidance Software for Percutaneous Access and Embolization of Type-II Endoleak after EVAR
Charudatta Bavare, MD, MPH, Ponraj Chinnadurai, MBBS, MMST, Christopher Smolock, MD, Joseph Naoum, MD, FACS, Heitham Hassoun, MD, Alan Lumsden, MD, FACS, Jean Bismuth, MD, FACS.
The Methodist Hospital, Houston, TX, USA.
OBJECTIVES:
To evaluate the technical feasibility and to illustrate the clinical workflow of using C-arm Computed Tomography (CT) (angio CT) and fluoroscopic needle guidance software, for percutaneous access and embolization of type-II endoleak after endovascular aortic aneurysm repair (EVAR).
METHODS:
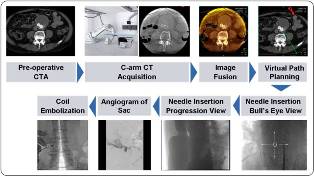
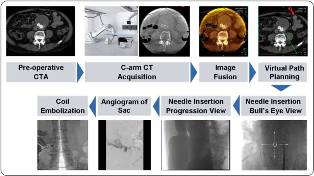
Between July 2010 and June 2011, fourteen cases of type II endoleak after EVAR were treated in our hybrid operating room using C-arm CT (Syngo DynaCT®, Siemens AG, Forchheim, Germany) and fluoroscopic needle guidance software (Syngo iGuide®, Siemens AG). DynaCT® images were acquired using our robotic C-arm system (Artis Zeego®, Siemens AG). After merging with the pre-op CT demonstrating the endoleak, a virtual needle path was designed using iGuide®. We describe a clinical workflow using DynaCT® and iGuide® as a stepwise process to successfully access the aneurysm sac in a controlled fashion, as outlined in Fig 1. Where possible, selective catheterization and embolization of the communicating vessel was done with coils and/or injection of Onyx® Liquid Embolic System (ev3 Endovascular Inc., Plymouth, MN). Obliteration of flow in the sac was otherwise performed by injection of Onyx®.
RESULTS:
The mean age was 75 years (Range 64-86). All sac punctures were done percutaneous at the first attempt. Direct cannulation of the communicating vessel was done in two patients (15.4%). Final sac angiogram and post-operative duplex at 24 hours demonstrated no further endoleaks in all but one patient (92.8% success). Early in our experience, one patient underwent a non-guided sac puncture due to non-availability of the iGuide®, which resulted in puncture of the endograft, leading to hemoperitoneum needing emergent laparotomy.
CONCLUSIONS:
Percutaneous sac access with real-time three-dimensional fluoroscopic needle guidance is a minimally invasive treatment for complex type II endoleaks after EVAR. Although direct catheterization of the communicating vessel is challenging due to the fluid/thrombus in the sac, safe access of the sac and obliteration of flow can be successfully achieved.
Figure 1:
An illustration of clinical workflow about using DynaCT® and iGuide® software for percutaneous access of type II endoleak after EVAR.
Back to Annual Symposium Program

|