|
|
 |
Back to Annual Symposium Program
Intracardiac Leiomyomatosis: A Case Report and Literature Review
Trisha Roy, BASc, MD Candidate1, Richard O'Connor, MD, FRCSC2, Ian McGilvray, MD, PhD, FRCSC3, Graham Roche-Nagle, MD, MBA, FRCSI, EBSQ-VASC3.
1University of Toronto, Toronto, ON, Canada, 2Credit Valley Hospital, Mississauga, ON, Canada, 3University Health Network, Toronto, ON, Canada.
OBJECTIVES:
Intravenous leiomyomatosis (IVL) is a rare smooth muscle tumour characterized by the unusual growth of uterine leiomyomas into pelvic veins. Although these tumours are benign, in some cases they can extend into the inferior vena cava (IVC) and right-sided heart chambers resulting in life-threatening consequences. There is growing recognition of this fatal condition but intracardiac leiomyomatosis (ICL) may still be under recognized. Kocica et al performed a literature review in 2005 of all reported cases of ICL. We present an updated extensive literature review of ICL from 2005-2011 and a case report illustrating features of this pathology.
METHODS:
We performed a comprehensive literature search using MEDLINE, Embase and PubMed databases using MeSH terms: “leiomyomatosis” and “heart”, limited to English articles from 2005 to 2011. References within each publication were searched to identify reported cases of ICL to date.
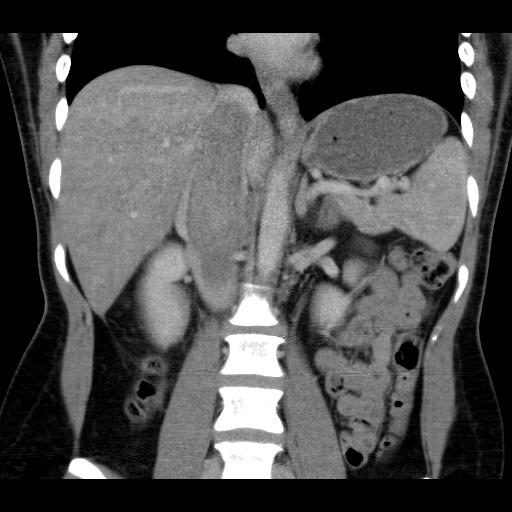
RESULTS:
We present a case of a 37-year-old female with ICL extending to the right atrium and treated with a one-stage tumour excision with perioperative TEE. This case demonstrates the important factors in diagnosis and management of this pathology. The literature search generated 41 published articles of 116 ICL cases from 2005-2011. There are a total of 229 cases of ICL reported from its first description in 1907. 51% of all ICL cases were reported from 2005-2011. Patients are on average 42.9 years old (20-72) and presented most often with symptoms of dyspnea, palpitations and syncope. The most commonly reported preoperative imaging techniques were CT and transthoracic echocardiogram (TTE). However, misdiagnoses on CT and TTE of atrial myxoma or atrial/IVC thrombus were reported in 10 cases. Radical excision is required because incomplete excision results in recurrences, as reported in 11 cases. Radical excision may be achieved via one-stage (60% of reported cases) or two-stage (40% of reported cases) operations. Perioperative TEE was reported in 5 cases and was a powerful tool for diagnosis and guiding surgical management.
CONCLUSIONS:
ICL may be an under recognized fatal condition that requires a high index of clinical suspicion. Contemporary imaging tools including TEE can aid in diagnosing ICL and guide optimal surgical strategy. 
Back to Annual Symposium Program

|