|
Back to Annual Meeting Program
Hospital Reimbursement for Carotid Stenting and Carotid Endarterectomy
Melissa J. Donovan, MD, Daniel E. Ramirez, MD, Gregory D. Crenshaw, MD, Taylor A. Smith, MD, Hernan A. Bazan, MD, W. Charles Sternbergh, III, MD.
Ochsner Medical Center, New Orleans, LA, USA.
Introduction: We have previously demonstrated that carotid artery stenting (CAS) had a 40% greater cost than carotid endarterectomy (CEA) and did not provide superior outcome or a reduction in length of stay. However, Medicare hospital reimbursement for CAS (DRGs 34,35,36) is 12-61% greater than that for CEA (DRGs 37,38,39). Hospital reimbursement for these procedures has not been previously examined.
Methods: A retrospective review of the hospital reimbursement and cost for CAS and CEA was performed over a 33 month period at a single tertiary care institution. This financial data was calculated through the institution’s Eclipsys cost accounting system, which captures hospital reimbursement as well as direct, variable and fixed costs. Physician professional fees and reimbursements were excluded. Data are presented as mean ± S.D.
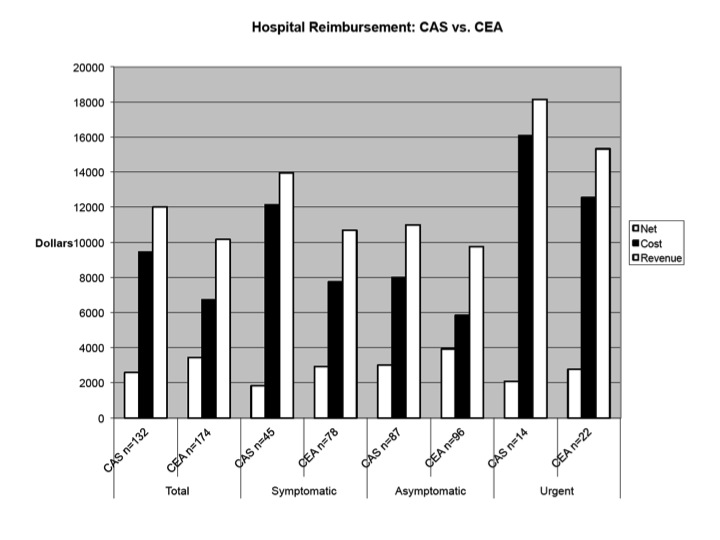
Results: 306 patients underwent CAS (n=132) or CEA (n=174). Hospital reimbursement was 18% higher for CAS ($12,000 ±5634) vs CEA ($10,160 ±4687), P <0.01. However, because of the significantly higher materials’ costs of CAS, the net revenue (income) for the hospital was 33% greater in patients undergoing CEA ($3426) than CAS ($2574) These differences in hospital reimbursement and net income were consistent in asymptomatic (n=183), symptomatic (n=123), , and urgent (n=36) subgroups (see Figure). Asymptomatic patients generated a higher net revenue than symptomatic patients whether undergoing CEA or CAS..
Conclusions: Hospital reimbursement for CAS was 18% higher than that for CEA. However, CEA was associated with a 33% higher net income because of the 40% cost premium of CAS. Asymptomatic patients have the lowest cost and highest net income of all the subgroups, likely due to less complex clinical presentation and associated testing. At present, CAS is not routinely cost-effective in a fee-for-service or capitated health care environment. 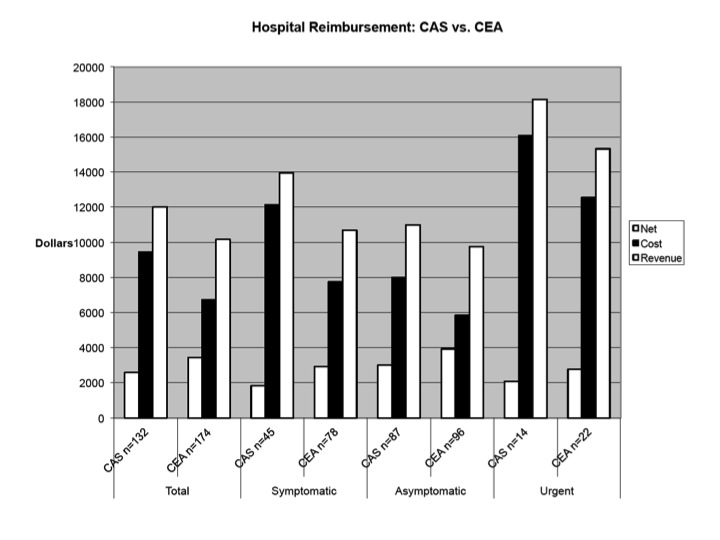
Back to Annual Meeting Program

|