|
Back to Annual Meeting Program
Surgical reconstruction of the cephalic arch for the management of dysfunctional brachiocephalic arteriovenous fistulas
Javier E. Anaya-Ayala, MD, Nader Zamani, BS, Nyla Ismail, PhD, Tony Lu, MD, Cassidy Duran, MD, Hosam F. El-Sayed, MD, Mark G. Davies, MD, PhD, MBA, Eric K. Peden, MD.
Methodist DeBakey Heart & Vascular Center, Houston, TX, USA.
Background: Development of recalcitrant stenotic lesions of the cephalic arch is a common failure mode of brachiocephalic arteriovenous fistulas. Endovascular treatment is the first line of therapy for cephalic arch stenosis (CeAS). Suboptimal outcomes have led to exploration of surgical alternatives. We evaluate our initial experience with a cephalic arch reconstruction to salvage malfunctioning brachiocephalic arteriovenous fistulas.
Methods: We did a retrospective review of all patient requiring surgical revision of a compromised brachiocephalic AVF due to CeAS. All patients had failed percutaneous interventions and underwent cephalic arch reconstruction (CAR) for salvage. Indications, clinical considerations and surgical technique were studied; initial patency, complications and reinterventions were reviewed.
Results: From April 2011 to July 2012, 15 patients (54% female mean age 55 +-22) underwent CAR. Stenotic lesions of the cephalic arch at the confluence with the axillary vein were confirmed by contrast venography. The average number of percutaneous interventions prior to the decision to CAR was 3 (range 2-7), the time from access creation to cephalic arch reconstruction was 33 months. Surgical approach involved revisions of the cephalic arch to re-direct the flow either as a direct reconnection to the axillary or as a turndown procedure to the brachial vein in the axilla. Technical success was 100%; all patients were able to use successfully their access for dialysis after the procedure. Two patients (13%) required angioplasty of the CAR due to restenosis, another patient required evacuation of hematoma in postoperative day 14. At a mean of 12 months follow up, all arteriovenous fistulas remain functional.
Conclusions: The initial experience with cephalic arch reconstruction demonstrates that is an effective surgical option to salvage brachiocephalic AVFs with excellent short-term and functional results. 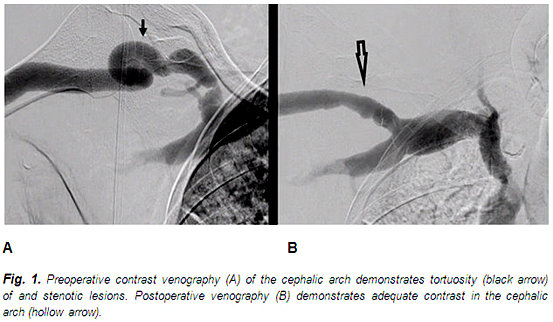
Back to Annual Meeting Program

|

