|
Back to Annual Meeting Posters
Duplex Scanning Alterations in Patients Treated with Endovascular Aortic Aneurysm Repair in the Stented Versus Snorkeled Renal Artery
Paul B. Haser, M.D., Wendy K. Fujioka, Saum A. Rahimi, MD, Tal Bash, M.D., Alan M. Graham, M.D..
Robert Wood Johnson Medical School, New Brunswick, NJ, USA.
OBJECTIVES:For patients undergoing abdominal aortic aneurysm (AAA) endovascular repair (EVAR) with short, proximal seal zones, renal artery stenting just above the EVAR or in parallel with the main graft, (the snorkel technique), provides alternative therapy to open surgery. However, a comparison between proximal aortic seal zone diameter changes and renal velocity duplex alterations has not previously been examined. In this study, we sought to determine the changes in the proximal neck and renal blood flow, especially concerning renal duplex scanning.
METHODS: In this single-institution, retrospective study, all patients who underwent EVAR between January 2003 and July 2012 were candidates for this study if they had at least one postoperative renal duplex scan and if a renal stent was placed either above (EVAR-stent) or in parallel to the EVAR (EVAR-snorkel). Data from each of the patient’s renal arteries was considered separately; CTA findings along with velocity trends with RD were tracked.
RESULTS: A total of 1,192 patients underwent an EVAR procedure and among these patients, 16 patients had at least one artery protected using the snorkel technique (EVAR - snorkel) and 11 belonged to the EVAR-stent group. Velocities between EVAR-snorkel (n=19, 12 stented and 7 native) and the EVAR-stent (n=21, 8 stented and 13 native) were statistically different (Table 1). CTA also documented a significantly wider proximal neck in the EVAR-snorkel group compared to the EVAR-stented group (+5.6±1.9mm vs. -1.17±5.5mm). Postoperative complications in the snorkeled patient population included: contained type 1 endoleak (n=4), type 2 endoleaks (n=6), and retroperitoneal hemorrhage (n=2). In the EVAR-stented patients, type 2 endoleak (n=4) was the most common complication. Duplex criteria for renal stenosis (> 50 %) was present in both the snorkeled (n=5) and stented (n=6) group, but only clinically significant in one EVAR-stent patient, requiring repeat angioplasty.
CONCLUSIONS:The snorkel and stenting techniques allows for endovascular treatment of aortic aneurysms with short proximal necks, but snorkeling appears to contribute to widening at the proximal seal zone, associated with increased, contained type 1 endoleaks. Renal duplex velocities are affected in not only the intervened-upon vessel, but also the contralateral, native vessel. 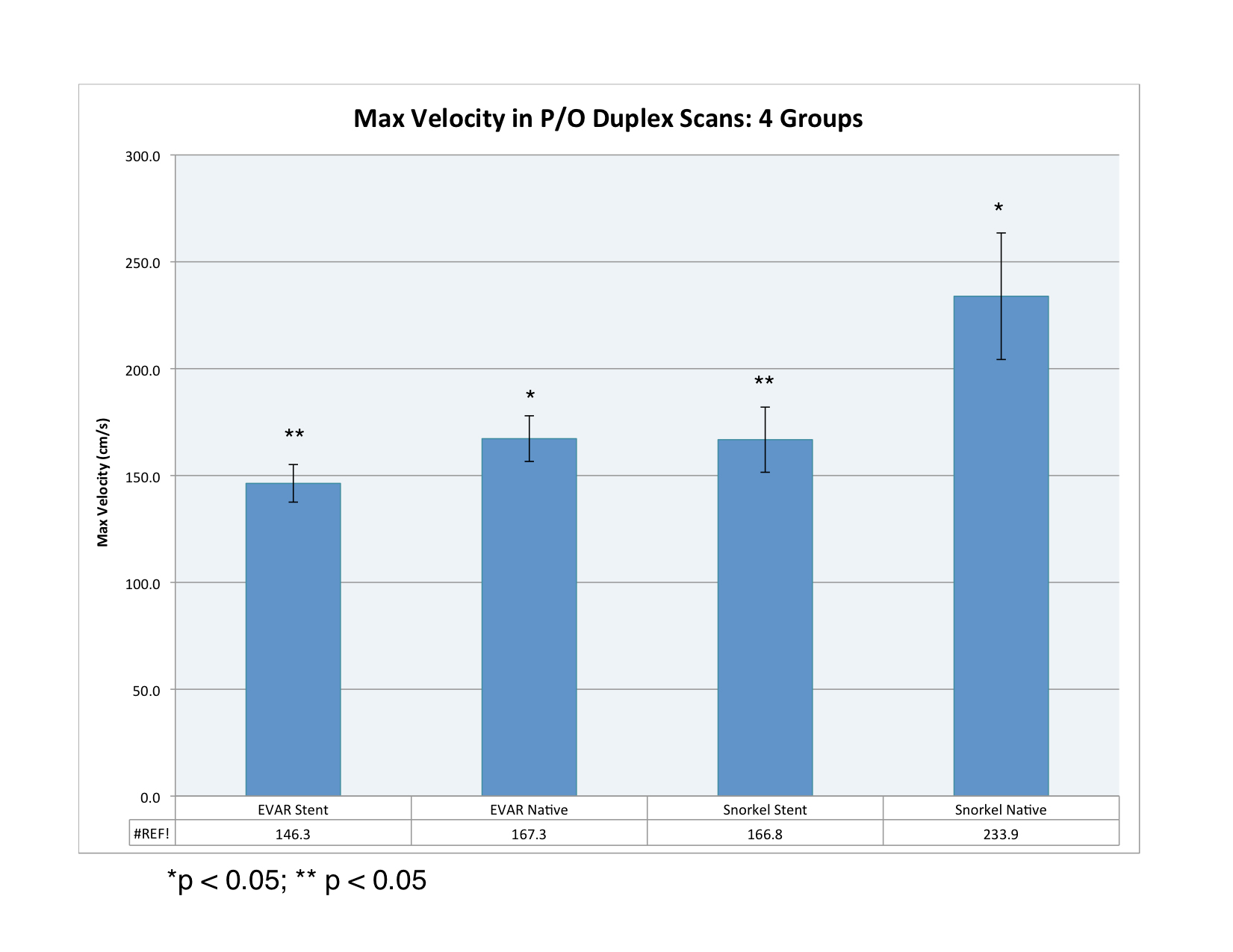
Back to Annual Meeting Posters

|
