|
|
 |
Back to Annual Meeting Posters
Early Experience with Endografts in the Ascending Aorta Suggests Avoiding Acute Dissection
Tulio P. Navarro, Sr., MD, PhD1, Rodrigo C. Bernardes, Sr., MD1, Fernando R. Reis, Sr., MD1, Luiz CM Lima, Sr., MD1, Ernesto L. Monteiro, Sr., MD1, Jose O. Leite, Sr., MD1, Francesco E. Botelho, Sr., MD1, Alan Dardik, Sr., MD, PhD2.
1Madre Teresa Hospital Aortic Center, Belo Horizonte, Brazil, 2Yale University School of Medicine, New haven, CT, USA.
<OBJECTIVES: Evaluate feasibility and outcomes of endografting ascending aorta in acute aortic syndromes.
METHODS: Six cases of acute aortic syndrome of the ascending aorta (2 dissections and 4 penetrating aortic ulcers) were treated by endograft placement, without branched or fenestrated devices, between December 2007 and September 2011.
RESULTS: The technical success rate was 83.3% (5 of 6). Intraoperative complications included one left carotid artery occlusion successfully treated by stenting and one death due to acute aortic valve dysfunction. Postoperative complications included aortic rupture in both patients that initially presented with acute dissection; both patients were treated with and survived emergency open surgery, with no major complications. During follow-up (mean 25.8 months), all patients are alive without any symptoms, without supra-aortic vessel occlusion, without aortic diameter growth and without any endoleaks.
CONCLUSIONS: Endograft treatment of the ascending aorta is feasible when the anatomy is suitable and may be an alternative to open repair, with reasonable midterm results, in patients with a penetrating aortic ulcer. However, both patients with acute aortic dissection had repeated dissection with aortic rupture despite endograft placement, suggesting that acute ascending aortic dissection may not be suitable for minimally invasive therapy. 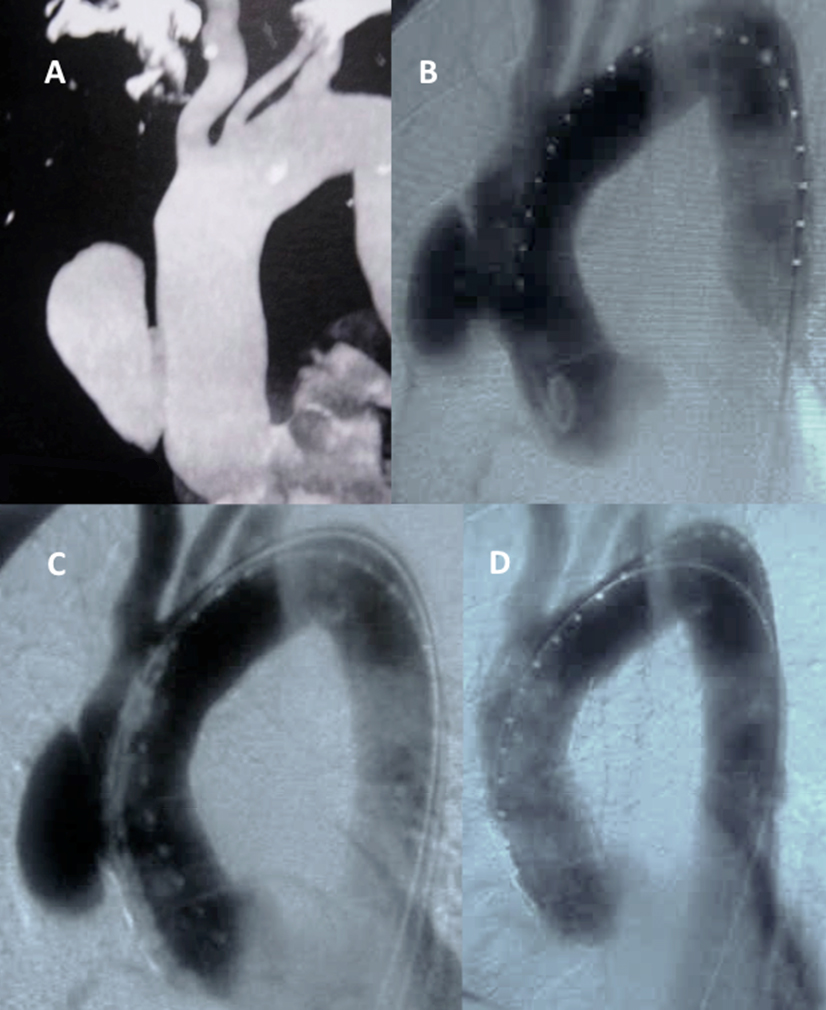
Figure 1: Treatment of an ascending aortic penetrating ulcer. (A) Computed tomography and (B) angiography showing a penetrating ulcer at the ascending aorta. (C) Positioning the thoracic TEVAR device between the ostia of the coronary arteries and the innominate artery. (D) Post deployment angiography depicting technical success. White arrow: Right coronary artery; Black arrow: Innominate artery.
Back to Annual Meeting Posters

|
