|
|
 |
Back to Annual Meeting Posters
Endovascular repair (EVAR) of ruptured abdominal aortic aneurysms (RAAA) improves outcome in octogenarians and in high risk patients
Mateus P. Correa, MD, Audra A. Duncan, MD, Andrew Bakken, MD, Manju Kalra, MBBS, Gustavo S. Oderich, MD, Mark Fleming, MD, Thomas C. Bower, MD, Peter Gloviczki, MD.
Mayo Clinic, Rochester, MN, USA.
Objectives: To review the current management strategies and outcomes in patients treated for RAAA in the EVAR era.
Methods: A retrospective review of consecutive patients with the diagnosis of RAAA between 1998 to 2010 was performed. This time period occurred prior to the institution of a protocol to facilitate EVAR repair of all RAAAs. Clinical variables affecting outcomes were univariately and multivariately analyzed.
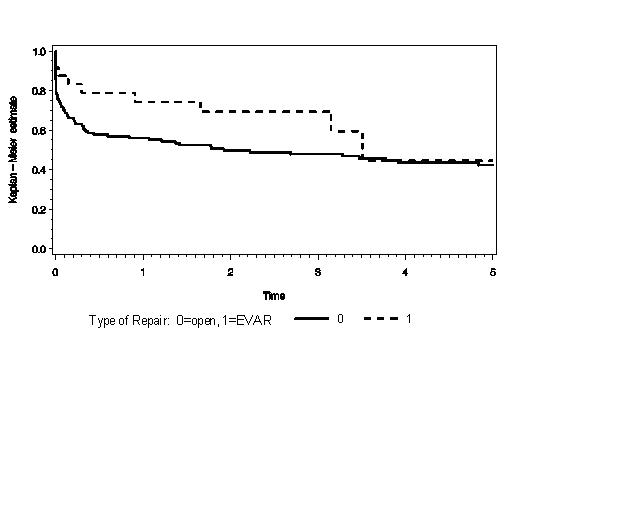
Results: 169 patients, 123 males and 34 females with a mean age of 75.5 years (range 34-95) were studied. 35% were older than 80 years of age. Three patients (1%) died before intervention and nine (5%) declined surgery. Of the remaining 157, EVAR was performed in 24 (15%) patients, and open repair (OR) in 133 (85%). 72 patients with OR were anatomically unsuitable for EVAR (57 patients with a short neck (mean length 9.0mm) or involvement of visceral arteries), 52 had no CT scan performed, and 12 had EVAR-suitable anatomy. Thirty-day and one-year mortality rates in the EVAR and OR groups were 12%/29% and 26%/44%, respectively (p-value 0.07). (Figure) Among OR patients, 30-day and 1-year mortality was the same with or without EVAR-suitable anatomy. EVAR patients’ mortality (3 of 24, 12%) compared to the mortality of OR in EVAR-suitable patient (3 of 12, 25%) p=0.36. Differences between the EVAR and OR groups include baseline hemoglobin (p=0.02) and death (p=0.04), whereas APACHE II scores were the same (p=0.2). Univariate analysis identified Apache II score, age, renal failure, and dialysis as predictors of death (p<.001). Age >80 years, suprarenal clamp and Apache II score were associated multivariately with 30-day mortality; age >80 years and Apache II score were associated with one-year mortality.
Conclusion: Our study suggests a trend that EVAR will reduce mortality in the short and mid-term, and confirms our current practice to perform EVAR in all RAAA if anatomically suitable. EVAR may particularly improve survival in RAAA patients over 80 or those with higher APACHE II scores. As suprarenal clamp was associated with 30-day mortality, further study is necessary to determine whether off-the-shelf branch grafts for juxtarenal or suprarenal aneurysms will improve RAAA survival.
Back to Annual Meeting Posters

|
