|
|
 |
Back to Annual Meeting Posters
Revisiting the Natural History of Aortic Aneurysms
Charles D. Salisbury, BS, Thomas C. Matthews, MD, Mark A. Patterson, MD, Marc A. Passman, MD, William D. Jordan, MD.
UAB, BIRMINGHAM, AL, USA.
Objective:
Aortic aneurysms (AA), when identified, are typically followed expectantly via defined surveillance protocols until repair is necessary. We sought to identify the natural history of surveillance in AA that meet size criteria for repair.
Methods:
All AA patients who were referred to our vascular group and followed with surveillance between 1996 and 2012 were identified from a prospectively maintained vascular registry. Health system charts, medical communication, and national death indexes were reviewed. Chi-square data analysis was performed and Kaplan-Meier survival curves were calculated.
Results:
Between January 1996 and June 2012, 885 patients were identified to have aortic aneurysms and never repaired. These patients were followed up to 190 months and the average length of surveillance was 29 months (range: 0.1 - 189.9). There were 81 thoracic aneurysms (TAA, 8.8%), 78 thoracoabdominal aortic aneurysms (TAAA, 9.2%), and 726 abdominal aortic aneurysms (AAA, 82.0%). Mean time of survival was 70.3, 51.8, and 43.4 months for AAA, TAA, and TAAA respectively. The reasons for surveillance included small aneurysms (n=624), medical risk (n=104), not endovascular candidates (93), and patient preference (64). The mean survival was 85.1, 21.1, 32.9, and 43.1 months, respectively. Out of the 885 patients that underwent surveillance, 430 (48.6%) of them died during the follow up period. Mortality was categorized as follows: unknown (n=243, 56.5%), malignancy (n=67, 15.6%), cardiovascular (n=42, 9.8%), pulmonary (n=17, 4.0%), aortic rupture (n=15, 3.5%), stroke (n=11, 2.6%), neurologic (n=10, 2.3%), renal failure (n=8, 1.9%), trauma (n=7, 1.6%), sepsis (n=7, 1.6%), and aortic dissection (n=3, 0.9%).
Conclusions:
Surveillance remains the standard of care for management of aortic aneurysms up to a certain size threshold. Long-term survival is greater for AAA compared to TAA or TAAA. Although the majority of patients died from non-aortic causes, a subset died from aortic rupture or dissection, supporting the known mortality risk for untreated aortic aneurysms that meet size criteria for repair. 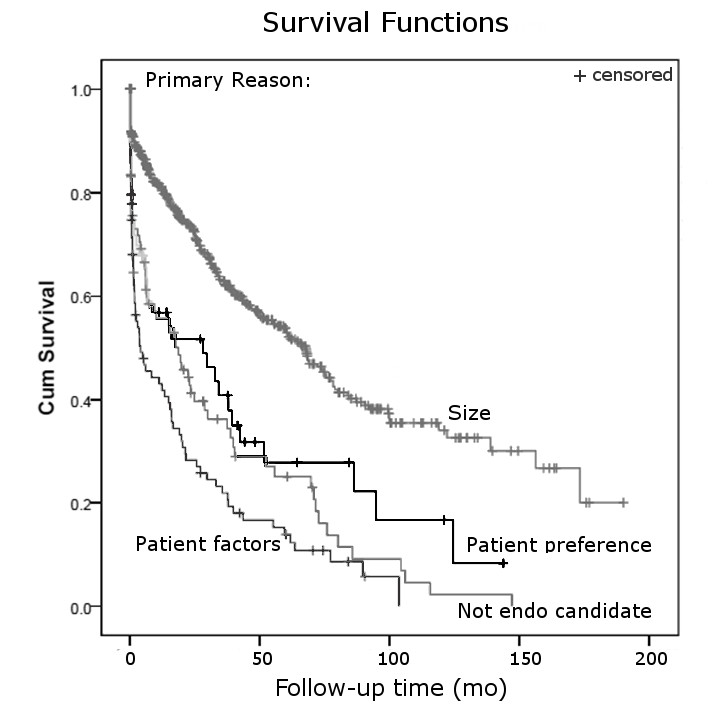
Back to Annual Meeting Posters

|
