|
Back to Annual Meeting Posters
Recurrent, Symptomatic Thoracic Aortic Mural Thrombus Following Open Thoracic Aortic Endarterectomy: Management by TEVAR.
John G. Maijub, M.D.1, Marvin E. Morris, M.D.1, Charles B. Ross, M.D.2.
1Norton Hospital, Louisville, KY, USA, 2Piedmont Heart Institute, Atlanta, GA, USA.
OBJECTIVES: Recurrent, symptomatic thoracic aortic mural thrombi (TAMT) following definitive operative management is rare. Treatment options include therapeutic anticoagulation, reoperative eradication of the offending thrombus, and exclusion by covering the lesion with a thoracic aortic endograft (TEVAR). There has been one reported case of TEVAR for early recurrent TAMT following operative treatment. We present the second reported case of symptomatic, recurrent TAMT, encountered two years following thoracic aortic endarterectomy performed for the identical clinical syndrome, managed by lesion exclusion with TEVAR.
METHODS: A 39 year old lady with known thrombophilic disorder presented with signs of acute left upper extremity and acute on chronic right lower extremity ischemia of embolic origin. After a trial of therapeutic anticoagulation, she underwent left posterolateral thoracotomy with aortic and left subclavian artery thrombectomy under left heart bypass. She represented almost two years later with evidence of left lower extremity rest pain and atheroembolization. Computed tomography angiography (CTA) confirmed recurrent TAMT in the descending thoracic aorta (Figure 1a-b).
RESULTS: Lysis of the thrombus was not achieved with a short trial of intravenous heparin. Given her propensity for embolization and considering her cardiovascular comorbidities and prior thoracotomy, percutaneous endovascular stent graft exclusion was performed with successful thrombus exclusion (Figure 1c). No complications were experienced in the immediate postoperative period, and she was discharged on postoperative day 3. She has had no further embolic events over the course of six months following TEVAR.
CONCLUSIONS: Management of symptomatic TAMT is dynamic and evolving. Management by exclusion utilizing thoracic aortic endografts is appropriate for recurrent TAMT and may well be appropriate primary management as well. 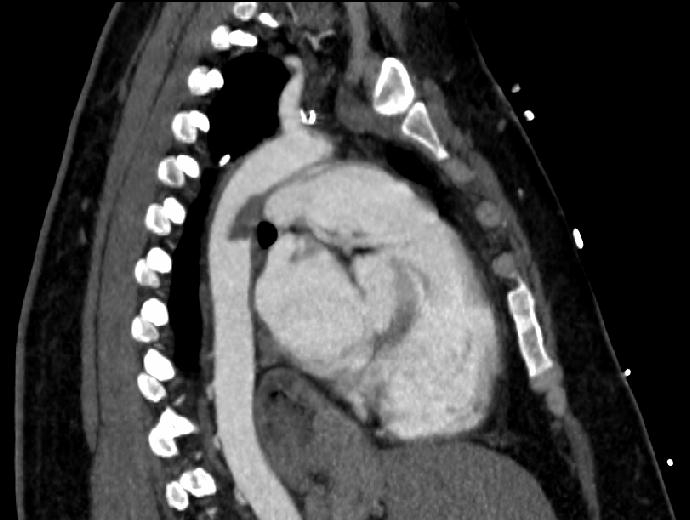  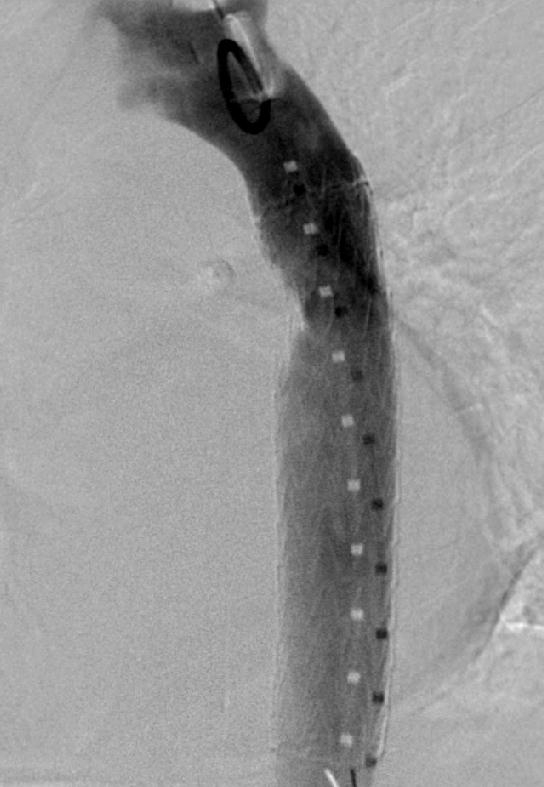
Back to Annual Meeting Posters

|
