|
Back to Annual Meeting Posters
Treatment of an Iatrogenic Abdominal Aortic Dissection with a Unibody Endograft
Jane K. Yang, M.D., Lee J. Goldstein, M.D., Arash Bornak, M.D..
University of Miami, Miller School of Medicine, Miami, FL, USA.
Objectives:
Complicated aortic dissections with acute lower extremity malperfusion have traditionally been treated with extra-anatomic revascularization or direct aortic surgery. In order to decrease the associated morbidity and mortality, endovascular techniques have been used over the last decade.
Iatrogenic dissection of the aorta is a steadily growing subgroup. We report the first known case in the literature of the endovascular treatment of an iatrogenic retrograde aorto-iliac dissection using a unibody endograft.
Methods:
A 45 year-old morbidly obese female (BMI 48.4) was referred for acute limb ischemia secondary to iatrogenic retrograde aorto-iliac dissection. The dissection occurred during percutaneous uterine fibroid embolization via right common femoral artery (CFA) access.
Her physical exam revealed absence of a right femoral artery pulse and an intermittent left femoral pulse, suggesting a dynamic aortic dissection flap.
An aortogram demonstrated bilateral renal perfusion and the true lumen of the distal aorta in continuity with the left common iliac artery (CIA), internal iliac artery (IIA) and external iliac artery (EIA). The right CIA was occluded with reconstitution of the distal EIA and IIA. The right CIA dissection flap was fenestrated and crossed from the left CFA access. The wire was then snared directly from the right CFA giving access to the true aortic lumen.
An AFX Unibody Endograft (Endologix, Irvine, CA) was deployed via the left CFA, covering the dynamic aortic flap and anatomically revascularizing bilateral CIAs. The right limb was extended with an iCast stent (Atrium Medical Corp., Hudson, NH) to cover the right CIA dissection.
Results:
Follow-up CT angiography at four months demonstrated patency of the endograft and adequate extremity perfusion.
This endovascular technique anatomically revascularized an aorto-iliac dissection. It covered a dynamic aortic flap that threatened patency of the aorta and the left iliac artery, while reestablishing bilateral lower extremity perfusion. Moreover, this technique allowed us to avoid an extra-anatomical bypass in this morbidly obese patient with its associated potential complications.
Conclusions:
The use of an aortic endograft is an alternative for treatment in a patient with an iatrogenic abdominal aortic and iliac artery dissection. It is feasible and preserves anatomical arterial circulation. 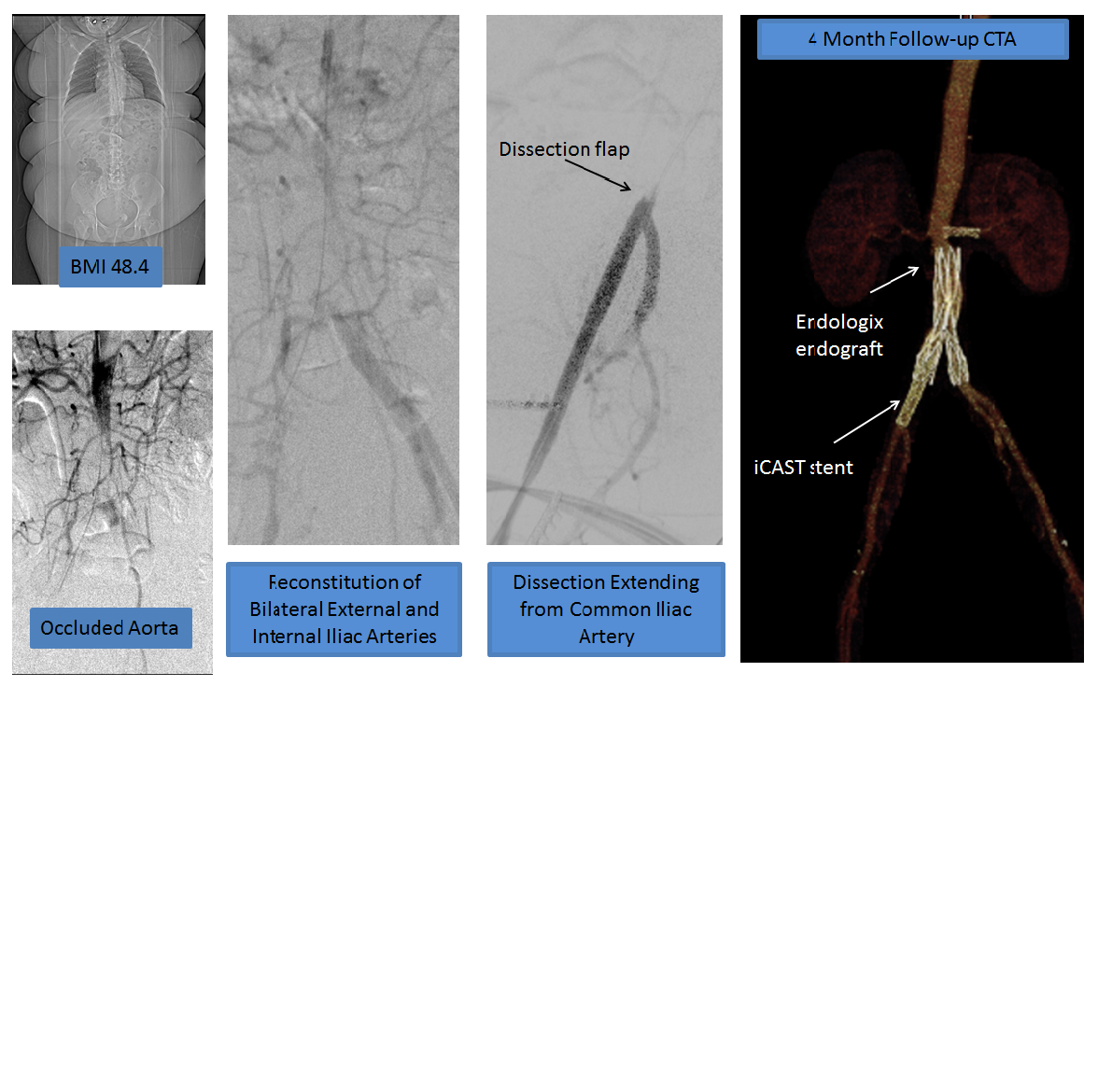
Back to Annual Meeting Posters

|
