|
Back to Annual Meeting Program
The decline of mesenteric ischemia-related mortality in the last decade
Ruby C. Lo, MD, Margriet Fokkema, MD, Thomas Curran, MD, Allen D. Hamdan, MD, Mark Wyers, MD, Marc L. Schermerhorn, MD.
Beth Israel Deaconess Medical Center, Boston, MA, USA.
BACKGROUND
Angioplasty and stenting (PTA/S) has been increasingly used for the treatment of mesenteric ischemia but whether this has decreased open revascularizations and/or improved overall mortality is unknown.
METHODS
Using the Nationwide Inpatient Sample from 1995 to 2010, we identified all admissions with a primary diagnosis of acute (AMI) or chronic (CMI) mesenteric ischemia that involved either PTA/S or open revascularization. We used the CDC’s Underlying Cause of Death database to confirm trends in AMI and CMI-related deaths and the continuous NHANES databases from 1999 to 2010 to describe patterns in cardiovascular medication use. Results were indexed to the population and expressed per 100,000 using U.S. Census Bureau data.
RESULTS
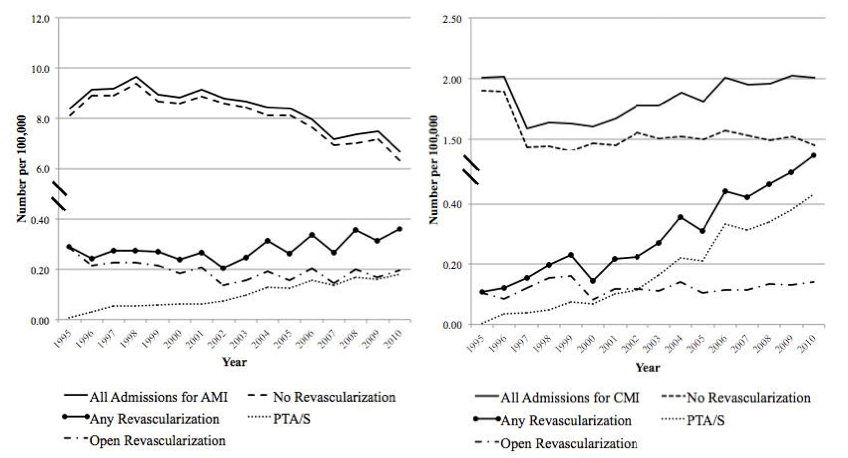
We identified 386,230 admissions for AMI and 85,016 for CMI during which 13,198 PTA/S (35% AMI) and 14,569 open revascularizations (62% AMI) were performed. Hospitalizations for AMI declined from 8.4 to 6.7 while those for CMI remained around 2.0 (Figure). Total revascularizations for AMI increased from 0.3 to 0.4 with PTA/S approaching but never surpassing open procedures. For CMI, total revascularizations also increased from 0.1 to 0.6, driven primarily by PTA/S. In-hospital mortality of patients undergoing repair declined from 51% to 26% for AMI and from 9% to 5% for CMI whereas mortality rates for patients without intervention also declined from 26% to 13% for AMI and from 8% to 6% for CMI. CDC data confirmed that deaths attributable to AMI have declined from 1.5 to 0.6 while those for CMI have remained stable around 0.1. NHANES data demonstrated that warfarin use increased from 86 to 211 and statin use from 555 to 1,455 per 100,000.
CONCLUSIONS
In the last decade, PTA/S increased without a concurrent decline in open revascularizations for both AMI and CMI. Meanwhile, in-hospital mortality has dropped regardless of acuity or repair approach. For CMI, this may be related to the performance of PTA/S in patients who would previously have been ineligible for surgery. The decline in deaths attributable to AMI has been dominated by a decreased incidence of AMI coinciding with increased warfarin use. In contrast, admissions for CMI have increased despite increasing statin use. 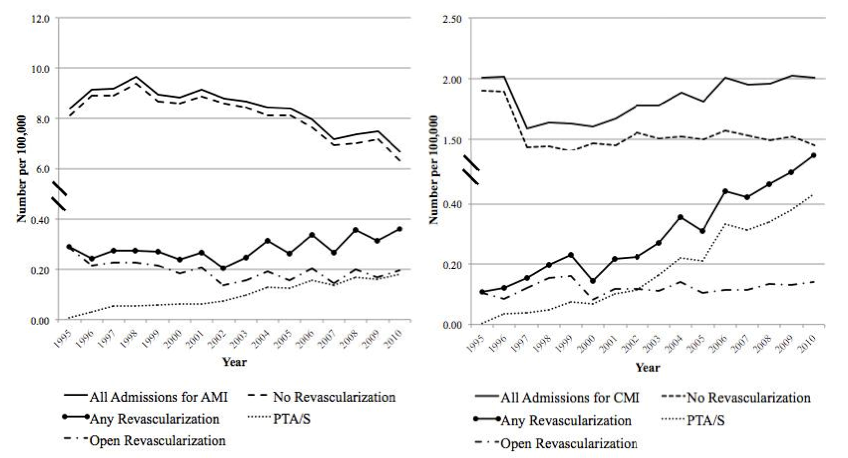
Back to Annual Meeting Program

|