|
|
 |
Back to Annual Meeting Program
Arterio-venous Grafts are Acceptable for Dialysis Patients with Limited Life Expectancy
Matthew T. Allemang, MD1, Brian Schmotzer, MS2, Virginia L. Wong, MD1, Alexander Chang, MD1, Ryan O. Lakin, MD1, Kenneth J. Woodside, MD1, John Wang, MD1, Vikram S. Kashyap, MD1.
1University Hospitals Case Medical Center, Cleveland, OH, USA, 2Case Western Reserve University, Cleveland, OH, USA.
OBJECTIVES:
To estimate the patency of arteriovenous fistulas (AVF) and grafts (AVG) for dialysis access in a tertiary care setting and understand clinical variables that affect outcomes.
METHODS:
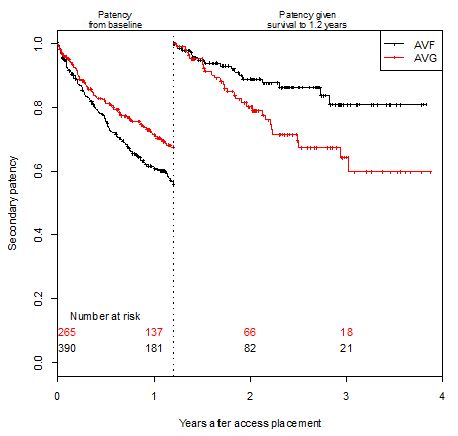
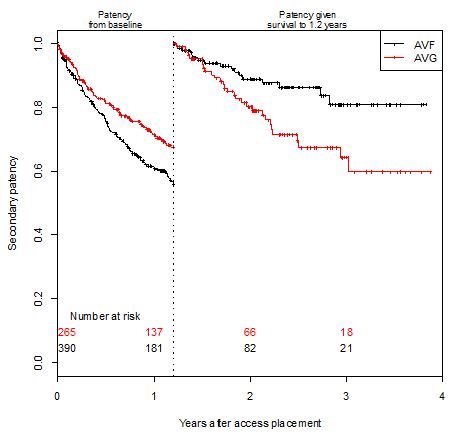
Records of patients who had a dialysis access placed from January 2008 until June 2011 were retrospectively reviewed. Outcomes were assisted primary patency and secondary patency. Marginal survival models (to account for correlation of accesses within subjects) utilizing Cox proportional hazard regression were used for statistical comparisons. The proportional hazards assumption was found to be met if the time course was bisected, resulting in separate hazard ratio (HR) estimates before and after 1.2 years.
RESULTS:
A total of 494 patients with 655 accesses (390 AVF, 265 AVG) were examined. 271 patients had only AVFs, 153 had only AVGs, and 70 had sequential AVF/AVG. The average age was 58.3 ± 16.4 for AVF and 60.8 ± 16.6 for AVG with 46% male, 72% African-American, 52% diabetic, and 66% with a tunneled catheter at the time of access placement. Seventy-seven percent of primary accesses (N=305) were "fistula-first". We found AVG were worse for both assisted primary patency and secondary patency (median 1 intervention) after 1.2 years (HR: 4.8 CI: (2.8, 8.3) and HR: 2.1 CI: (1.2, 3.9), respectively). However, from time of placement until 1.2 years, secondary patency for AVGs was better (HR: 0.7 CI: (0.5 to 0.9)) while assisted primary patency was worse (HR: 1.4 CI: (1.1, 1.8)). Kaplan-Meier estimates for secondary patency before and after the 1.2 year cutoff were constructed (Figure). In a multivariable model including age, diabetes, PVD, ever used tobacco, previous access placement, and tunneled catheter, the HR for AVG was 0.6 (CI: 0.4, 0.8) before 1.2 years. Other results were also similar in the multivariable model.
CONCLUSIONS:
AV grafts can be maintained with high rates of secondary patency in the short-term, but are not as durable in the long-term. Patients with limited life expectancy can effectively be offered an AV graft when native veins are of limited quality for fistula construction.
Back to Annual Meeting Program

|