|
Back to Annual Meeting Posters
Hemodialysis aAcess in the Elderly: Do the Results Justify Following the KDOQI Guidelines?
Houssam K. Younes, MD, Charudatta Bavare, MD, Mitul S. Patel, MD, Abindra Sigdel, MD, Jospeh J. Naoum, MD, Hosam F. El-Sayed, MD, Eric K. Peden, MD, Mark G. Davies, MD.
Methodist DeBakey Heart and Vascular Center. The Methodist Hospital, Houston, TX, USA.
OBJECTIVES:The KDOQI guidelines have succeeded in increasing fistula implantation as long term dialysis access. However, the role of these guidelines in the elderly population (>70yrs old) is unclear. The aim of this study is to examine the outcomes of access creation in the elderly population in relation to KDOQI
METHODS:
We retrospectively reviewed all patients that were older than 70 years old who underwent upper extremity arteriovenous fistula (AVF) or graft (AVG) creation at our dialysis access center between 2006-2010. Kaplan-Meier method was used to calculate primary, assisted-primary and secondary patency rates. The patency rates were compared with the log-rank test. Complication and intervention rates were compared using Chi Square test.
RESULTS:
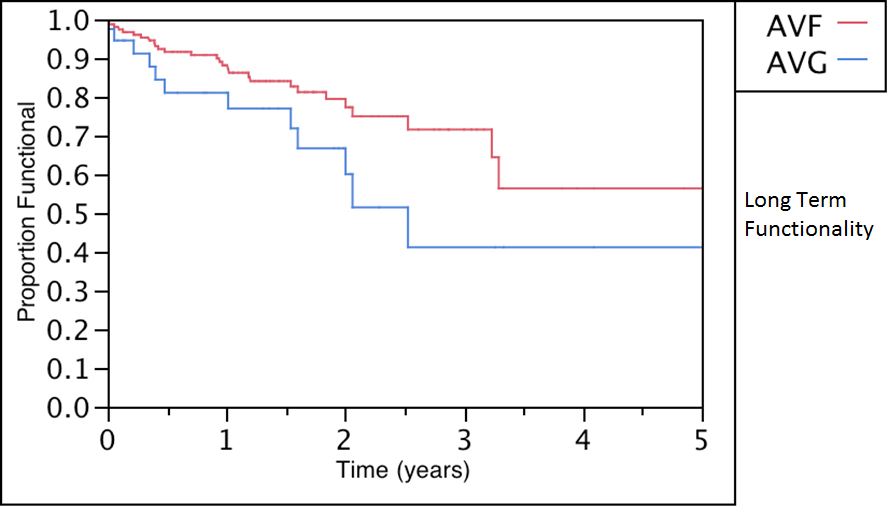
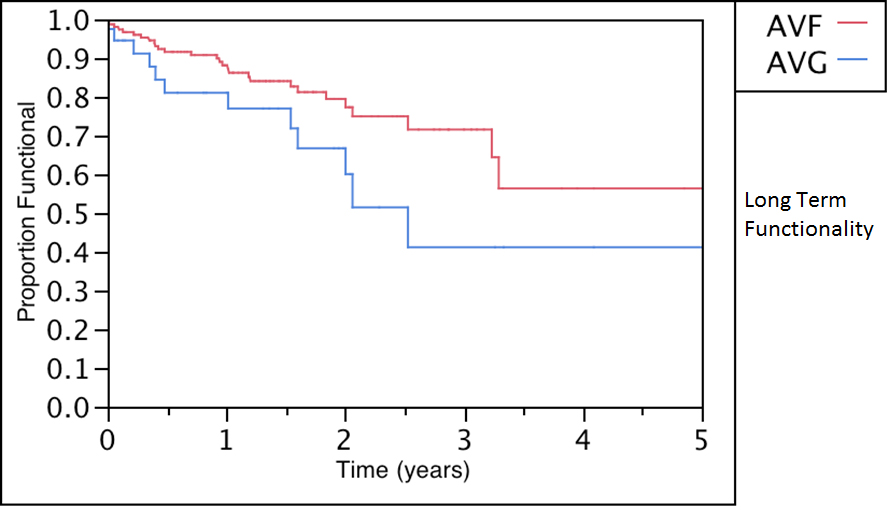
161 elderly patients underwent access creation (121 AVF and 40 AVG). 52% were male with a mean age of 74yrs (range 70-91). Their mean SVS morbidity score was 6. The 30 days mortality is 0.02% and 0.05 % for AVF and AVG respectively. During follow-up, there was a trend towards improved primary 1-year and 5 years patency rates for the AVF over AVG: (88±3% vs 81±8% at 1 yr and 56±1% vs 41±13% at 5yrs , AVF vs. AVG, P = 0.06). Secondary patency were comparable in both groups; (56±1% vs 41±13%, AVF vs. AVG, P = 0.06). Long term functionality for both access types is shown in the figure. The incidence rate of complications was 1.52 vs 3.86 per patient in the AVF and AVG groups respectively (P<0.05). Patients with AVF required a total of 1.03 interventions per patient vs 3.85 per patient for the AVG group (P<0.05). 0.025% of the patients with AVF and 0.05 % of patients with AVG required a second access creation before death.
CONCLUSIONS:
Hemodialysis access whether it is an AVF or an AVG in the elderly patient results in comparable patency and functionality. They generally only require one successful access creation. However, as would be expected AVGs are associated with increased number of complications and
significantly more interventions during follow up.
Back to Annual Meeting Posters

|