|
|
 |
Back to Annual Meeting Posters
Wound Infection Following Open Aortic Surgery Correlates With Trunk Muscle Size
Shipra Arya, MD, SM, Brandon M. Wojcik, MD, Shijie Cai, BA, Michael Terjimanian, BA, Jay Lee, BA, Jordan Starr, BA, John E. Rectenwald, MD, MS, Michael Englesbe, MD, Jonathan L. Eliason, MD, Katherine A. Gallagher, MD.
University of Michigan, Ann Arbor, MI, USA.
Objectives: Infection is a significant cause of morbidity and mortality in vascular surgery patients undergoing open aortic surgery. Identifying patients at risk for infectious complications pre-operatively may facilitate improved post-surgical outcomes. The purpose of the current study was to determine whether pre-operative trunk muscle size on computed tomography (CT) was associated with increased wound infection rates following open aortic surgery.
Methods: The medical records of 482 patients who underwent elective open AAA repair at our tertiary care center between 2000 and 2009 were queried. 260 had pre-operative CT imaging within 90 days of surgery suitable for analysis. Cross-sectional area of the psoas muscles was measured at the L4 vertebral level, with additional subcutaneous fat measurements obtained. Data pertaining to demographics, preoperative variables and post-operative morbidity and mortality were obtained. Associations between pre-operative factors including total psoas area (TPA) and early and late wound infection rates were assessed using Cox regression analysis.
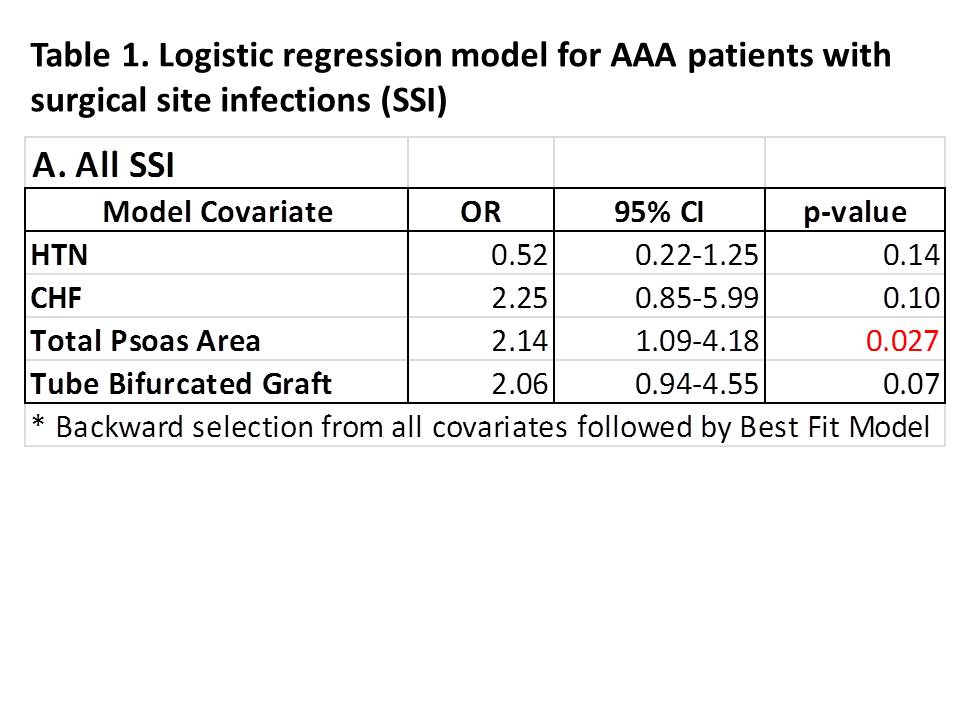
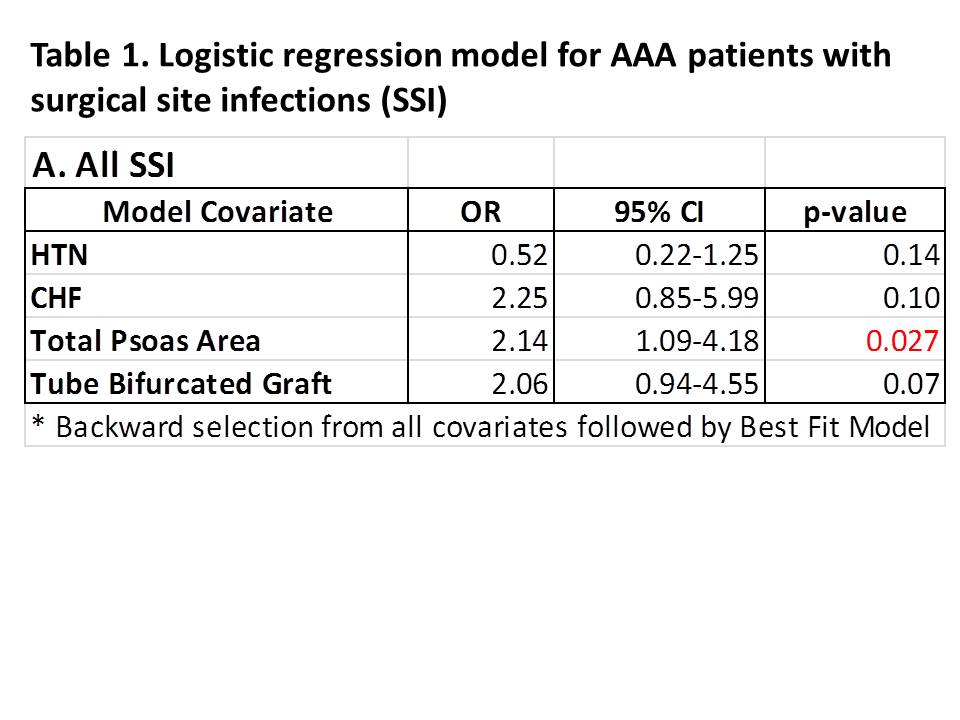
Results: The mean age of our cohort was 70 years (27% female). Hypertension (78%), hyperlipidemia (64%), COPD (38%) and smoking (92%) were the most prevalent pre-operative risk factors. There were no significant differences in the comorbid conditions, BMI (mean 28) or demographics with respect to development of an SSI. Bifurcated grafts were used in 30% of the patients, and were associated with a higher risk of SSI on univariate analysis. With a mean follow-up of 5.45 years, deep and superficial infections were observed in 11.9% of AAA patients. 9.2% developed early (<30 days) infections while 7% developed late infections. Morphometric analysis demonstrated that increased TPA was associated with the development of a wound infection by both univariate (p=.019) and multivariate (p=.02; OR=2.14) analysis (Table 1). No significant differences were noted with respect to subcutaneous fat area. Significant differences in mortality were noted on KM survival curves at 5 years following SSI.
Conclusions: Pre-operative core muscle size by CT has a strong association with the development of wound infections following open AAA surgery. Morphometric analysis may aid in risk stratification for patients undergoing open aortic surgery.
Back to Annual Meeting Posters

|