Back to Annual Meeting Symposium
Shuttering of the Superior Mesenteric Artery During Fenestrated EVAR
Brant W. Ullery, M.D., George K. Lee, M.D., Jason T. Lee, M.D..
Stanford University, Stanford, CA, USA.
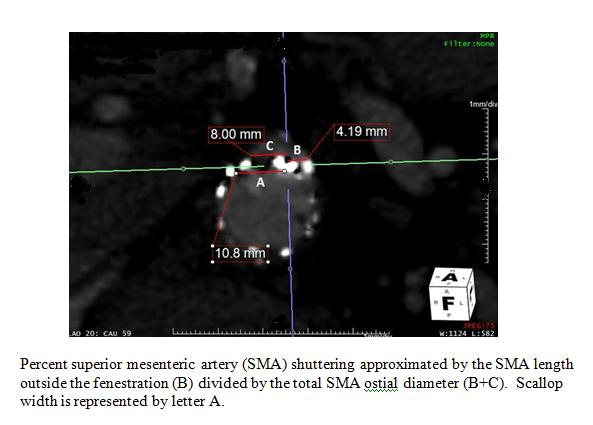
OBJECTIVES: Shuttering occurs when a scallop or fenestration
does not align perfectly with the target vessel ostium, and is potentially
minimized by stenting. The currently approved fenestrated endovascular aortic repair (f-EVAR) platform usually utilizes a non-stented superior mesenteric artery (SMA) scallop, thereby subjecting the SMA to risk of partial coverage. We sought to describe the presence and degree of SMA shuttering during f-EVAR.<
METHODS: Patients undergoing f-EVAR using the commercially available ZFEN device containing an SMA scallop at our institution were included for analysis. Corrected multiplanar coronal images on postoperative CT-A were reviewed to measure SMA shuttering, defined as the percentage of SMA ostial diameter covered by the stent-graft fabric (Figure).
RESULTS: Of the 24 f-EVAR cases performed during the study period, 14 patients had an SMA scallop to include in this analysis (male, 71%; mean age, 75 years; mean AAA size, 6.4 cm). Thirty-nine vessels were targeted (14 SMA scallops, 25 renal fenestrations), with covered stents placed in all fenestrations. Target vessel catheterization was achieved in 100% of cases. SMA shuttering of any amount occurred in 64% of patients (range, 24%-54%). Degree of SMA shuttering varied: no patients had 1-20%, four had 21-40%, and five had 41-60%. All celiac and SMA vessels were patent on postoperative imaging. On univariate analysis, there was no association between SMA shuttering and the measured clock position of the SMA or renal arteries, percent of device oversizing, number of renal artery fenestrations/stents, aneurysm neck morphology, or aortic diameter at the SMA or proximal seal. No clinical events of mesenteric ischemia were noted in any of the patients.
CONCLUSIONS: Even with the custom design of currently available fenestrated technology, shuttering of the SMA occurs in more than half of the patients, although no clinical events were noted. Further detail with regards to the incidence, magnitude, and tolerance of SMA shuttering during f-EVAR is warranted to fully understand the clinical implication of this radiographic finding. Future design considerations for advanced EVAR should take into account SMA shuttering to further refine operative planning.
Back to Annual Meeting Symposium

|
