Back to Annual Meeting Symposium
Comparison of a Vascular Study Group of New England (VSGNE) Risk Prediction Model With the Established Risk Prediction Models of In-Hospital Mortality After Elective Abdominal Aortic Aneurysm (AAA) Repair
Mohammad H. Eslami, MD1, Denis Rybin, PhD2, Gheorghe Doros, PhD2, Jeffrey Kalish, MD1, Alik Farber, MD1.
1Boston University School of Medicine, Boston, MA, USA, 2Boston University School of Public Health, Boston, MA, USA.
Introduction: Elective AAA repair can lead to in-hospital mortality, but no agreement exists on the most accurate predictive model for in-hospital mortality. The purpose of this study was to develop a risk prediction model using VSGNE data and compare that to established models.
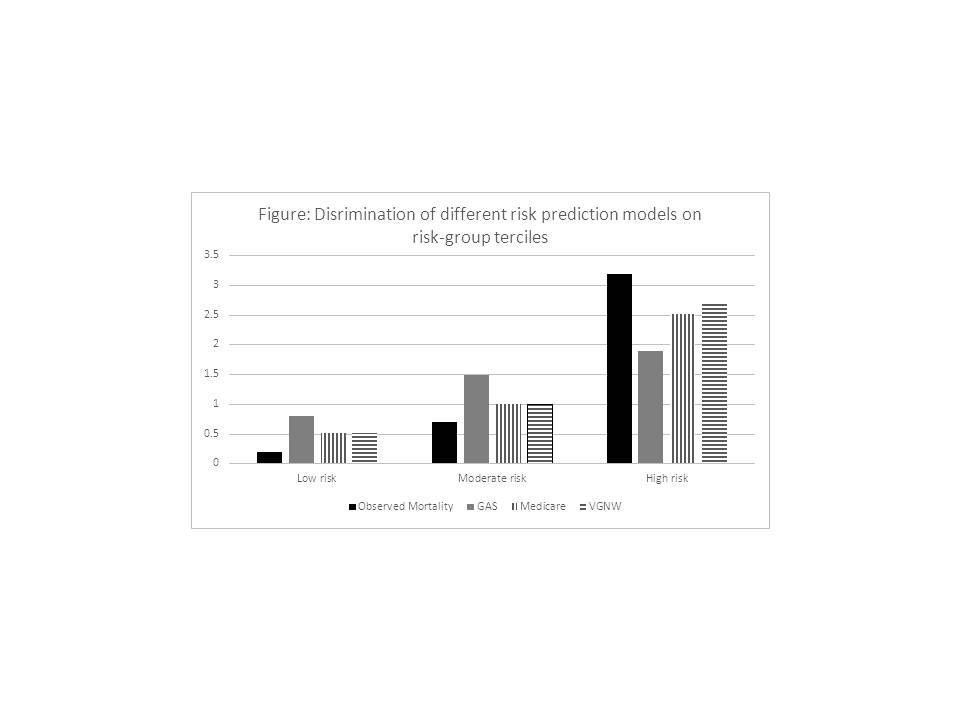
Methods: VSGNE data (2003-2013) was queried for patients undergoing elective AAA repair by open (OAR) or endovascular (EVAR) techniques. Clinical variables including known predictors of mortality were included in a full prediction model. Backward elimination with alpha-level of 0.5 was used to construct a parsimonious model. This model (VSGNE) was then compared to established models based on the scope of VSGNE data collection: Medicare, Glasgow Aneurysm Score (GAS) and Vascular Governance North West (VGNW). Vuong test was performed to compare the fit of models. Model discrimination was compared in equally-sized risk-group VSGNE terciles.
Results: The overall mortality rate for 4597 elective AAA patients was 1.5%, with a significantly higher mortality rate for OAR (2.7% vs. 0.7%, p<.001). Table below shows the parsimonious model. The discriminating ability of the VSGNE model was high(C-statistic=0.812) and corrected slightly to 0.782 after internal validation. Vuong tests yielded significant overall fit difference favoring VSGNE model over all three models and Medicare(C-statistic 0.761) and VGNW (0.760) to GAS (0.681). VGNW and Medicare models performed better than GAS in predicting mortality among risk-group terciles (Figure).
Conclusion: The VSGNE risk prediction model forecasts mortality the best among this patient population. Both Medicare and VGNW models showed good discrimination.
Table: In-hospital Mortality after Elective AAA: Parsimonious 0.5 level (C=0.812) | | | | | | Adj. Odds Ratio | Lower Confidence Limit | Upper Confidence Limit | p value | | Open Infrarenal/Above One Renal Clamp vs. Endo | 3.8700 | 2.0485 | 7.3112 | <0.0001 | | Open Above Both Renals/Supraceliac Clamp vs. Endo | 8.6776 | 4.3051 | 17.4910 | <0.0001 | | Age | 1.0790 | 1.0368 | 1.1228 | 0.0002 | | Female vs. Male | 1.7280 | 1.0023 | 2.9794 | 0.0491 | | BMI | 0.9749 | 0.9260 | 1.0264 | 0.3337 | | Current Smoking: Yes vs. No | 0.6942 | 0.3065 | 1.5720 | 0.3814 | | Myocardial Disease | 1.7219 | 1.0019 | 2.9593 | 0.0492 | | CVD | 2.0902 | 0.9933 | 4.3984 | 0.0521 | | CHF | 1.7298 | 0.8520 | 3.5122 | 0.1294 | | COPD | 2.4737 | 1.4262 | 4.2905 | 0.0013 | | Creatinine | 1.3210 | 0.9575 | 1.8225 | 0.09 |
Back to Annual Meeting Symposium

|
