|
|
 |
Back to Annual Meeting Symposium
Trends in the Utilization and Cost of Ambulatory Endovascular Procedures
Thomas Curran, MD, John McCallum, MD, Dominique Buck, MD, Jeremy Darling, BA, Raul J. Guzman, MD, Mark Wyers, MD, Allen Hamdan, MD, Elliot Chaikof, MD, PhD, Marc Schermerhorn, MD.
Beth Israel Deaconess Medical Center, Boston, MA, USA.
OBJECTIVES:
Endovascular therapy is used increasingly for the treatment of claudication and limb threat (PAD). These procedures may be performed in the inpatient, hospital associated ambulatory or freestanding ambulatory settings though utilization and costs in the ambulatory setting have not been studied. We aim to evaluate trends in the utilization and cost of endovascular procedures across healthcare settings.
METHODS:
The State Ambulatory Surgery Databases (SASD) and State Inpatient Databases (SID) of Florida, New Jersey, California and Maryland from 2005 to 2009 were queried for patients undergoing elective endovascular procedures for PAD. Utilization trends for these procedures were stratified by indication {claudication vs. critical limb ischemia (CLI)} and service location (freestanding ambulatory, hospital associated ambulatory, inpatient). As freestanding data was available for Florida only, comparison of healthcare charges across locations was restricted to this state. Inpatient charges for cases with length of stay > 1 day were excluded from cost analysis.
RESULTS:
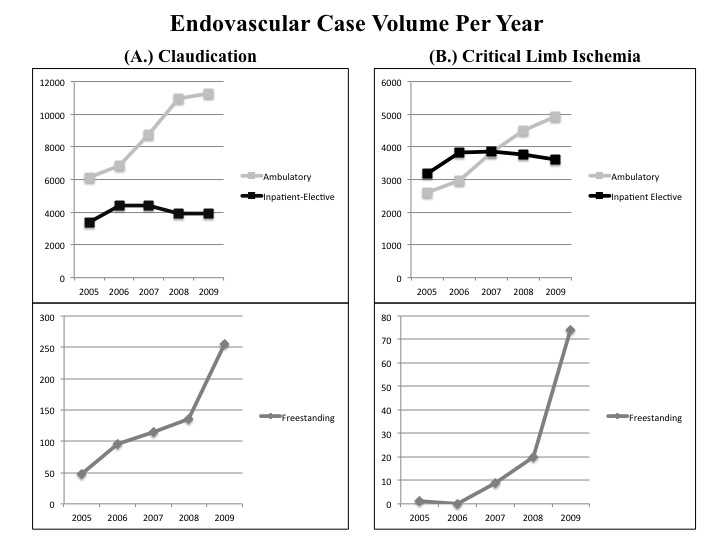
We identified 101,910 procedures; 64,722 (64%) for claudication and 37,188 (36%) for CLI. Overall procedure volume increased 57% from 2005 to 2009. Utilization of ambulatory facilities (freestanding and hospital associated) for claudication increased 84% from 2005 to 2009 (6,188 to 11,547) while inpatient procedures declined 11% from peak utilization in 2007 to 2009 (4,421 to 3,947). Freestanding procedures for claudication showed most pronounced increase with 444% (47 to 256) over the study period. Procedures for CLI increased in all service locations (Ambulatory: 2606 to 4936, 89%; Inpatient: 3173 to 3619, 14%). Total charges for treatment of claudication in freestanding centers were only 53% of hospital associated ambulatory centers ($14,727 vs. $27,945) while total charges for treatment of CLI were similar in freestanding vs. hospital associated ambulatory centers ($26,704 vs. $27,072). Inpatient charges far exceeded both ambulatory locations (Claudication: $39,900; CLI: $41,368).
CONCLUSIONS:
Freestanding and hospital associated ambulatory endovascular procedure utilization are increasing for both claudication and CLI. Treatment of claudicants in freestanding centers appears to be particularly cost effective.
Back to Annual Meeting Symposium

|
