|
|
 |
Back to Annual Symposium Program
The increased use of CTA and MRA as the sole imaging modalities prior to infrainguinal bypass has had no effect on outcomes
Bing Shue, MD1, Rachelle N. Damle, MD1, Jeffrey A. Kalish, MD2, David H. Stone, MD3, Virendra I. Patel, MD4, Andres Schanzer, MD1, Donald T. Baril, MD5.
1University of Massachusetts Medical School, Worcester, MA, USA, 2Boston Medical Center, Boston, MA, USA, 3Dartmouth Hitchcock Medical Center, Lebanon, NH, USA, 4Massachusetts General Hospital, Boston, MA, USA, 5University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
Objective: Angiography remains the gold standard imaging modality prior to infrainguinal bypass. Computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have emerged as non-invasive alternatives for pre-operative imaging. We sought to examine contemporary trends in the utilization of CTA and MRA as isolated imaging modalities prior to infrainguinal bypass and to compare outcomes following infrainguinal bypass in patients who underwent CTA or MRA versus those who underwent conventional angiography.
Methods: Patients undergoing infrainguinal bypass within the Vascular Study Group of New England were identified (2003-2012) Patients were stratified by pre-operative imaging modality: CTA/MRA alone or conventional angiography. Trends in utilization of these modalities were examined and demographics of these groups were compared. Primary end points included primary patency, secondary patency, and major adverse limb events (MALE) at 1-year as determined by Kaplan-Meier analysis. Multivariable Cox proportional hazards models were constructed to evaluate the effect of imaging modality on primary patency, secondary patency, and MALE.
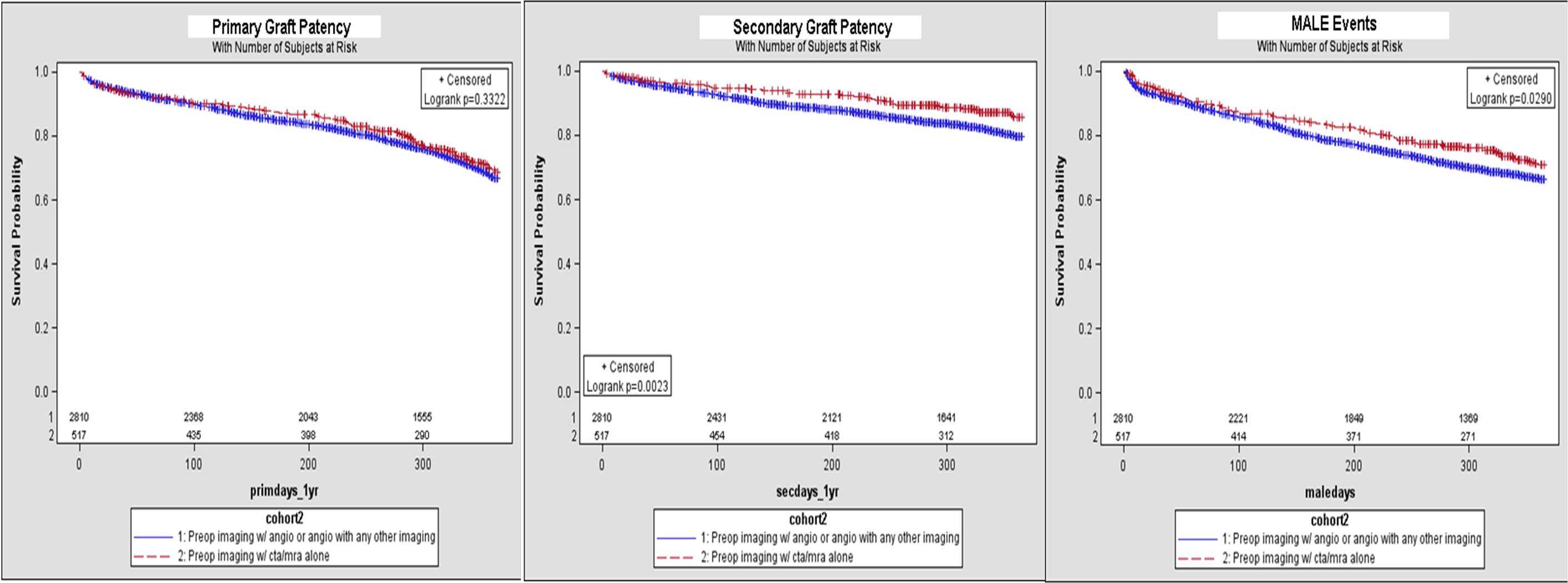
Results: In 3327 infrainguinal bypasses, CTA/MRA alone was used in 517 cases(15%) and angiography was used in 2810 cases(85%). In the CTA/MRA group, CTA was used more frequently than MRA(82% vs. 18%). Use of CTA/MRA alone increased over time, with 58(11%) bypasses from 2003-2005, 215(42%) bypasses from 2006-2009, and 244(47%) bypasses from 2010-2012 (P<0.001). Patients with CTA/MRA alone, compared to patients with angiography, more frequently underwent bypass for claudication (31% vs. 25%,P=0.0004) or acute limb ischemia (14% vs. 5%,P<0.0001), had aneurysmal disease (10% vs. 5%,P<0.0001), and less frequently had undergone a prior endovascular intervention (20% vs. 30%,P<0.0001). These patients more frequently had prosthetic conduits utilized (36% vs. 29%,P=0.001), and less frequently had tibial/pedal targets (31% vs. 40%,P=0.0002). After adjusting for confounders, multivariable analysis demonstrated that use of CTA/MRA alone was not associated with a significant difference in 1-year primary patency (HR 0.97; 95% CI, 0.80-1.17;P=0.74), secondary patency (HR 1.31; 95% CI, 1.00-1.72;P=0.05), or MALE (HR 1.08; CI 0.90-1.31;P=0.41)(FIGURE).
Conclusion: CTA and MRA are being increasingly utilized as the sole preoperative imaging modality prior to infrainguinal bypass. This shift in practice patterns appears to have no measurable effect on outcomes at 1-year.
Back to Annual Symposium Program

|
