|
Back to 2015 Annual Symposium Program
Endovascular Repair of Ruptured Abdominal Aortic Aneurysms does not Independently Reduce Long-Term Mortality Compared to Open Repair
William P. Robinson, MD, Andres Schanzer, MD, Francesco Aiello, MD, Julie Flahive, MS, Danielle R. Doucet, MD, Jessica P. Simons, MD, MPH, Elias Arous, MD, Louis M. Messina, MD.
University of Massachusetts Medical School, Worcester, MA, USA.
Objective: Endovascular repair (EVAR) of ruptured abdominal aortic aneurysms (RAAA) reduces in-hospital mortality compared to open repair (OR) but it is unknown whether EVAR reduces long-term mortality. We hypothesized that EVAR of RAAA would independently reduce long-term mortality compared to OR.
Methods: The Vascular Quality Initiative (VQI) database (2003-2013) was used to determine Kaplan-Meier 1-year and 5-year mortality after EVAR and OR of RAAA. Multivariate analysis was performed to identify patient and operative characteristics associated with mortality at 1 and 5 years after RAAA repair.
Results: Among 590 patients who underwent EVAR and 692 patients who underwent OR of RAAA, the lower mortality seen in-hospital after EVAR (EVAR: 23% vs. OR: 35%, p<0.001) persisted at 1-year (EVAR: 34% vs. OR: 42%, p=0.001) and 5 years (EVAR: 50% vs. OR: 58%, p=0.003, Figure) after repair. After adjusting for patient and operative characteristics, EVAR did not independently reduce mortality at 1 year (HR .88 [.7-1.1]) or 5 years (HR .95 [.77-1.2]) compared to OR. Women (HR 1.3 [1.04-1.6]), age (HR 1.06 [1.05-1.08] per 5 years), home oxygen use (HR 1.9 [1.3-2.7]), dialysis-dependence (HR 3.9 [1.8-8.6]), cardiac ejection fraction <50 % (HR 1.5 [1.03-2.1]), as well as preoperative systolic blood pressure< 90 mmHg (HR 1.4 [1.1-1.8]), loss of consciousness (HR 1.7 [1.3-2.2]), and cardiac arrest (HR 3.4 [2.5-4.5]) on admission predicted mortality at 1 and 5 years after RAAA repair. Type I endoleak (HR 2.2 [1.2-3.8]) also predicted mortality at 1 year.
Conclusions: EVAR does not independently reduce long-term mortality compared to OR. Patient comorbidities and indices of shock on admission are the primary independent determinants of long-term mortality. However, the lower early mortality observed in the VQI for patients selected to undergo EVAR of RAAA compared to patients selected for OR is sustained over time, supporting the use of EVAR for RAAA in appropriate candidates. Better elucidation of the key selection factors, including aneurysm anatomy, is needed to best select patients for EVAR and OR in order to reduce long-term mortality. 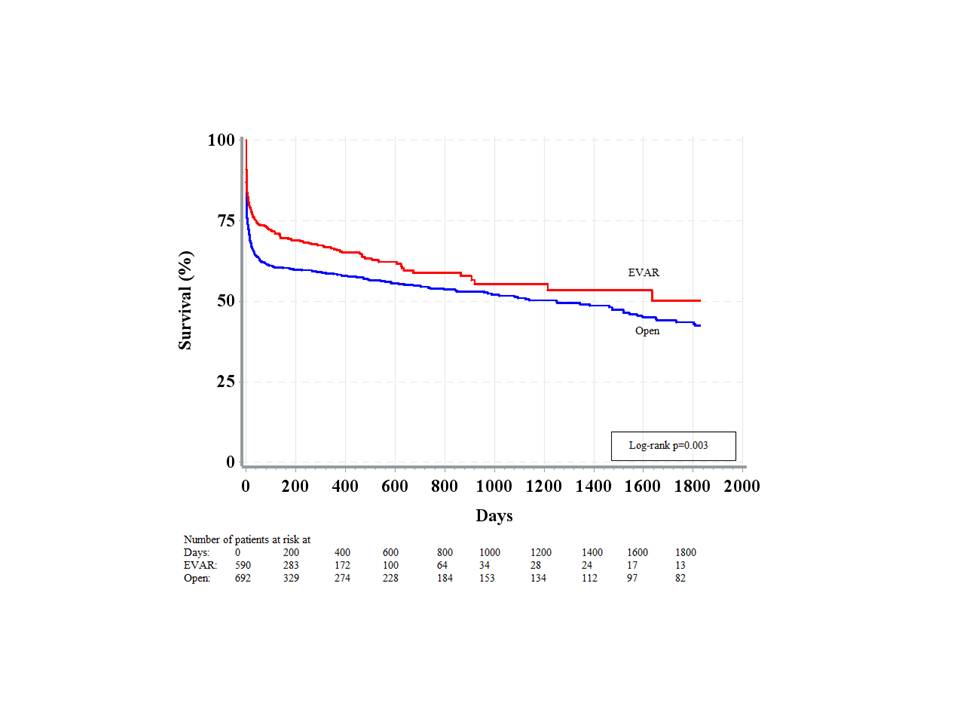
Back to 2015 Annual Symposium Program
|






