Back to 2015 Annual Symposium Program
Tibial Bypass Fails to Improve Healing Time of Wounds Compared to Serial Endovascular Tibial Intervention
Andrew M. Reittinger, Samuel N. Steerman, M.D..
Eastern Virginia Medical School, Norfolk, VA, USA.
Objective
Critical limb ischemia (CLI) has been traditionally treated with bypass surgery, but studies indicate that endovascular techniques can be a safe, effective method of revascularization. Subsequent intervention is often required in CLI patients that had previously undergone initial percutaneous treatment and the superiority of repeat endovascular interventions or tibial bypass is not clear in these patients.
Methods
A retrospective study was performed of all patients who underwent multiple tibial revascularizations for CLI from 1/1/2000 to 9/24/2013. All patients underwent endovascular tibial interventions as the initial procedure. The Tibial Bypass (TB) group included patients that had a tibial bypass as the second procedure. The Multiple Endovascular Interventions (MEI) group included patients treated with repeat endovascular tibial intervention. Group demographics, procedural data and outcomes were compared using t-test and Kaplan-Meier survival analysis.
Results
The TB group and MEI group included 32 and 181 patients, respectively. The groups were similar in demographics, medications, and risk factors. The MEI group had an average of 1.35 percutaneous revascularizations, with 5 being the maximum. Pre-operative indications for intervention were rest pain (TB 25.00% vs MEI 19.34%, p=0.464), ulceration (37.51% vs 47.50%, p=0.297), and gangrene (21.88% vs 20.99%, p=0.911). Average pre-operative Rutherford scores for the TB group and MEI group were comparable (4.774 vs 4.879, p=0.440). Tibial disease within the TB and MEI Groups was classified as TASC A (6.25% vs 7.73%, p=0.629), TASC B (34.38% vs 38.67%, p=0.646), TASC C (3.13% vs 14.36%, p=0.079), and TASC D (53.13% vs 19.89%, p<0.0001) after initial angiogram. The TB and MEI groups were followed for an average of 568.47 days and 453.84 days (p=0.161) after the final intervention, respectively. There were no significant differences between TB and MEI in mortality (18.8% vs 24.9%, p=0.458), post-operative complications (21.9% vs 15.5%, p=0.370), major amputation (28.1% vs 30.4%, p=0.802), minor amputation (32.3% vs 34.6%, p=0.802), ulcer healing rate (TB: 260.54 days vs MEI: 355.86 days, p=0.328, Figure) or ulcers healed (TB: 59.10% vs MEI: 46.15%, p=0.258).
Conclusions
After initial endovascular tibial intervention, performing multiple endovascular tibial interventions produces a rate of wound healing and limb salvage equal to lower extremity bypass. 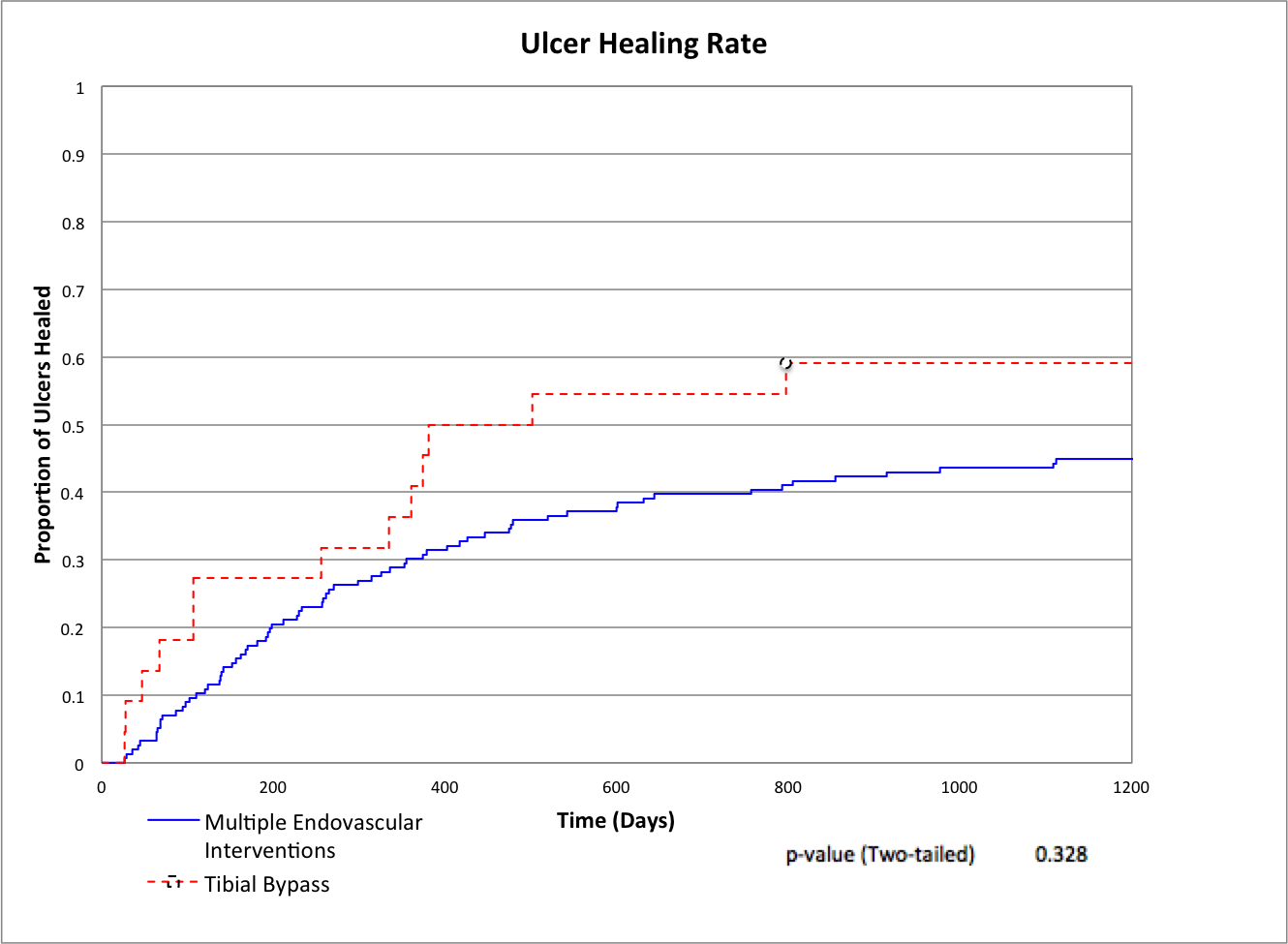
Back to 2015 Annual Symposium Program
|






