Back to 2015 Annual Symposium Program
Prognostication of Ruptured Abdominal Aortic Aneurysm Repair Using an Artificial Neural Network
Eric S. Wise, M.D., Kyle Hocking, Ph.D., Colleen Brophy, M.D..
Vanderbilt University, Nashville, TN, USA.
Objective:
First responders attending to ruptured abdominal aortic aneurysm (rAAA) patients relay pertinent information to anticipating providers prior to hospital transfer. Early identification of characteristics portending a poor outcome may prevent unnecessary operations and provide improved prognostic information. Artificial neural networks (ANN) are advanced, continually adapting computational systems taught to identify complex non-linear relationships among variables correlated with an outcome, with superior discriminant ability. Using ANN methodology, this study modeled in-hospital mortality after rAAA repair as a function of independent pre-operative predictors. We then developed a simplified ANN in which only variables most easily obtained prior to patient arrival can be used to accurately predict in-hospital mortality.
Methods:
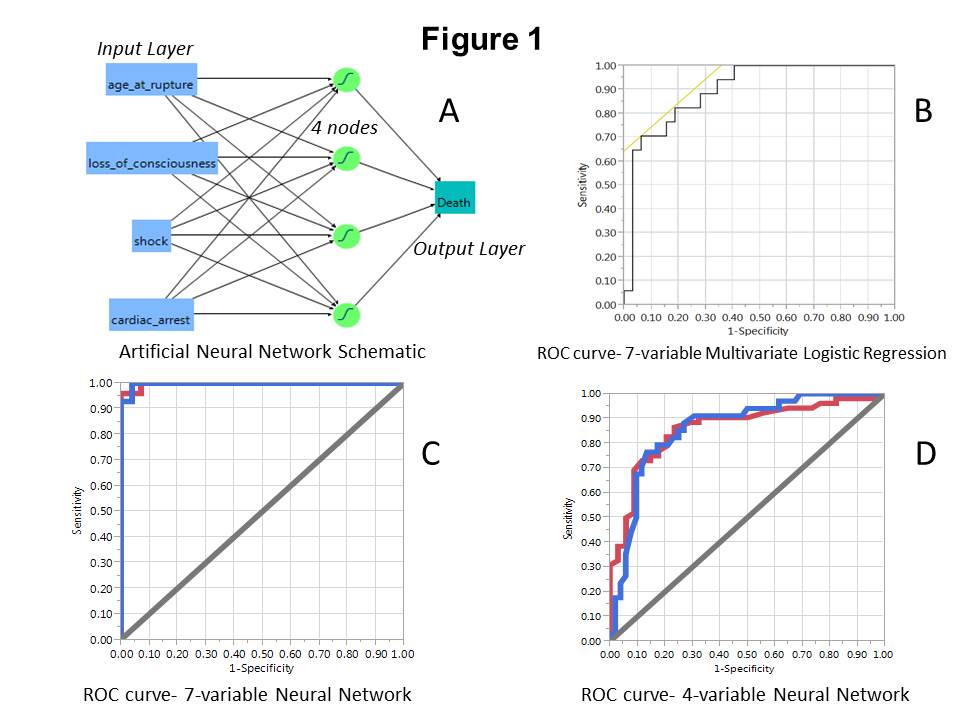
125 patients from 1998-2013 who had rAAA repair were reviewed for factors correlated with in-hospital mortality. Seven variables were significant in multivariate regression analysis (MRA); these variables were input into a computational ANN. Four of the pre-operative variables: age, shock, GCS <15 and cardiac arrest, chosen for their simplicity and ease of availability, were input into a second ANN (ANN-4, Figure 1A). MRA and ANN models were compared against the Glasgow Aneurysm Score (GAS). Models were assessed with a validation cohort, and by ROC-curve generation, with area under the curve (AUC) as the primary measure of each model’s discriminant ability.
Results:
Of the 125 patients, 53 (42%) did not survive to discharge. Seven pre-operative factors were significant (P<.05) independent predictors of mortality: age, elevated lactate, myocardial disease, acute or chronic renal failure, GCS<15, cardiac arrest and shock. After modeling these seven factors via MRA and ANN, the generated AUC’s were 0.8971±0.06 and 0.9971±0.004 (Figures 1B and 1C), respectively. In ANN-4, the AUC values were 0.8617±0.06 (Figure 1D) and 0.9259±0.05 in training and validation cohorts, respectively. Using an ANN output >0.5 for predicted death, ANN-4 discriminated with 86.5% sensitivity and 76.5% specificity. GAS fits the dataset with an AUC of 0.7666±0.06.
Conclusion:
ANN modeling represents a novel adjunct to the surgeon’s clinical judgment in rAAA patient management. Patients known to be elderly, in shock, requiring CPR and with GCS<15 may represent a cohort for whom attempted repair of rAAA carries little survival benefit.
Back to 2015 Annual Symposium Program
|






