|
Back to 2015 Annual Symposium Program
Multidisciplinary Approach to Vascular Surgery Coding Improves Coding Accuracy and Revenue Capture.
Francesco A. Aiello, M.D.1, Dejah Judelson, M.D.1, Jeffrey Indes, M.D.2, Sareh Rajaee, M.D.2, Louis Messina, M.D.1, Gordon Fitzgerald, PhD1, William Robinson, III, M.D.1, Danielle Doucet, M.D.1, Jessica Simons, M.D.1, Andres Schanzer, M.D.1.
1University of Massachusetts, Worcester, MA, USA, 2Yale University, New Haven, CT, USA.
OBJECTIVES:
Determine if a multidisciplinary approach to coding fistulagrams utilizing vascular surgeons and coders will improve coding accuracy and revenue capture.
METHODS:
This prospective observational study evaluates coding accuracy of fistulagrams at two large academic institutions (A and B). All fistulagrams were coded by hospital coders (traditional coding) and a single vascular surgeon whose codes were reviewed and verified by two coders at each institution(multidisciplinary coding). Both coding methods were compared and differences were translated into revenue ($) and work relative value units (wRVUs) using Medicare physician fee schedule. Comparison between traditional coding and multidisciplinary coding was performed for three discrete study periods at institution B: baseline (Period 1), after coding education session alone (Period 2) and after coding education plus implementation of operative note dictation template (Period 3). Accuracy of surgeon operative dictations were also assessed over each study period.
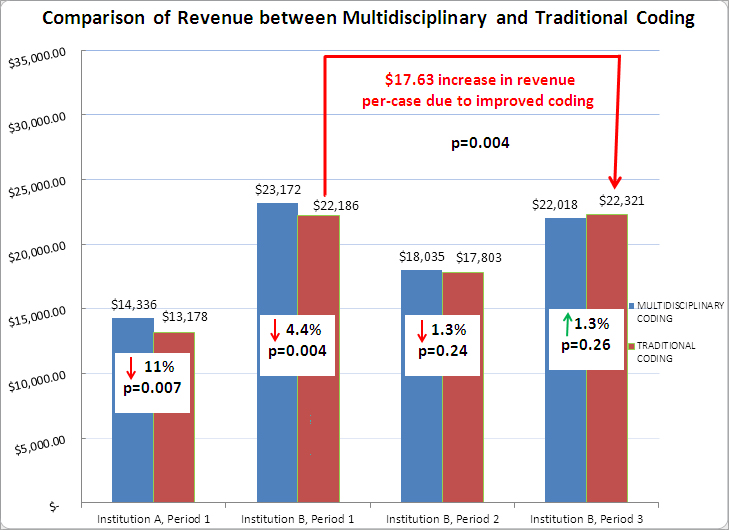
RESULTS:
During Period 1, traditional coding showed an 11% (p=0.007) loss in revenue and 12% (p=0.01) loss in wRVU generation at Institution A compared to multidisciplinary coding. At Institution B, traditional coding resulted in a 4.5% (p=0.004) loss in revenue and 5.5% (p=0.01) loss in wRVUs. During Period 2 at Institution B, there was no significant difference between traditional and multidisciplinary coding in revenue (1.3%, p=0.24) or wRVU generation (1.8%, p=0.20). During Period 3, traditional coding yielded a slightly higher overall revenue (1.3%, p=0.26) compared to multidisciplinary coding. This, however, was due to a 3.7% coding error by hospital coders with one missed code and five inappropriately used codes resulting in a higher overall reimbursement which was inaccurate and subsequently corrected. Assessment of physician documentation showed improvement over each study period with decreased documentation errors (11% vs. 3.1% vs. 0.7%, p=0.02) at each interval. Overall, comparison of traditional coding between periods 1 and 3 revealed improvements in revenue per-case ($17.63/case, p=0.004) and wRVUs(0.50/case, p=0.01).
CONCLUSIONS:
The use of a multidisciplinary coding system resulted in more accurate coding of fistulagrams with significant improvement in revenue and wRVU generation. If multidisciplinary coding across other endovascular procedures could yield similar improvements, this coding methodology would result in substantial increases in revenue capture.
Back to 2015 Annual Symposium Program
|






