Back to 2015 Annual Symposium Program
Comparative Occupational Radiation Exposure between Fixed and Mobile Imaging Systems
Daniel Kendrick, MD, Claire Miller, BS, Elizabeth Kudlaty, MS, Henry Baele, MD, Pamela Moorehead, BS, Ann Kim, MD, Dave Jordan, PhD, Vikram S. Kashyap, MD.
University Hospitals Case Medical Center, Cleveland, OH, USA.
OBJECTIVES:
Endovascular intervention exposes surgical staff to scatter radiation, which varies by procedure and imaging equipment. The purpose of this study is to determine differences in occupational exposure between procedures performed with fixed imaging (FI) in an endovascular suite compared to conventional mobile imaging (MI) in a standard operating room.
METHODS:
A series of 116 endovascular cases were performed over a 4-month interval in a dedicated endovascular suite with FI and conventional operating room with MI. All cases were performed at a single institution and radiation dose was recorded using real-time dosimetry badges from Unfors RaySafe™. A dosimeter was mounted in each room to establish a radiation baseline. Staff dose was recorded using individual badges worn on the torso lead. Total mean Kar (mGy, patient dose) and mean case dose (mSv, scatter radiation) were compared between rooms and across all staff positions for cases of varying complexity. Statistical analyses for all continuous variables were performed using t-test and ANOVA where appropriate.
RESULTS:
A total of 43 cases with MI and 73 cases with FI were performed by four vascular surgeons. Total mean Kar, and case dose, were significantly higher with FI when compared to MI. (mean ±SEM; 523 ±49mGy vs. 98 ±19 mGy; p<.00001; .77 ±.03 mSv vs. .16 ±.08 mSv, p<.00001). Exposure for both primary surgeon and assistant was significantly higher with FI compared to MI. Mean exposure for all cases using either imaging modality, was significantly higher for primary surgeons and assistant than for support staff beyond six feet from the X-ray source, indicated by one-way ANOVA (MI, p<.00001, PI, p<.00001). 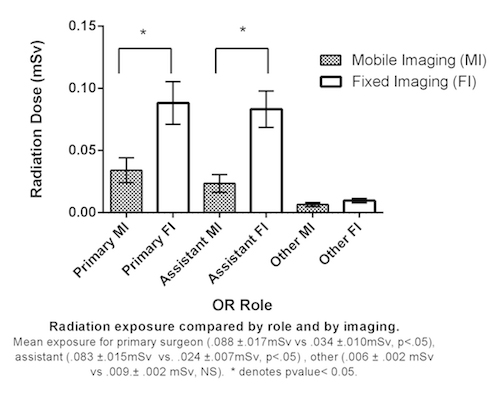 Support staff exposure was negligible and did not differ between FI and MI. Room dose stratified by case complexity (Kar) showed statistically significantly higher scatter radiation in FI vs. PI across all quartiles. Support staff exposure was negligible and did not differ between FI and MI. Room dose stratified by case complexity (Kar) showed statistically significantly higher scatter radiation in FI vs. PI across all quartiles.
CONCLUSIONS:
The generation of damaging scatter radiation is multiple-fold higher with FI than MI across all levels of case complexity. Dose exposure increases with proximity to the radiation source, and is negligible outside a six-foot radius. Modern endovascular suites allow high-fidelity imaging, yet additional strategies to minimize exposure and occupational risk are needed.
Back to 2015 Annual Symposium Program
|






