Back to 2015 Annual Symposium Program
A Novel Anatomic Severity Grading Score for Acute Type B Aortic Dissections and Correlation to Aortic Reinterventions after Thoracic Endovascular Aortic Repair
Shirui Chen, BA, Sebastian Larion, MS, S. Sadie Ahanchi, MD, Chad P. Ammar, MD, Colin T. Brandt, MD, Jean M. Panneton, MD.
Eastern Virginia Medical School, Norfolk, VA, USA.
Objectives:We introduce a novel preoperative anatomic severity grading (ASG) system for acute type B aortic dissections and test the system with a cohort of patients who underwent thoracic endovascular aortic repair (TEVAR).
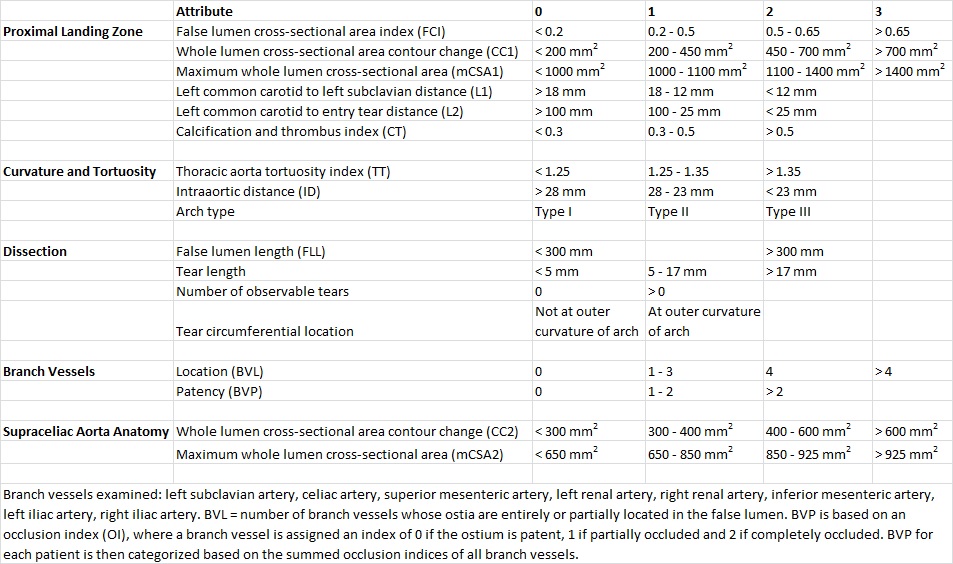
Methods:A cohort of patients who received TEVAR for acute type B aortic dissection between 2008-2014 was identified. We developed an ASG score to measure aspects of aortic anatomy that we hypothesized may affect difficulty of repair (shown below). We also calculated a false lumen volume index (FLVI=false lumen volume divided by the sum of the true and false lumen volumes). Measurements were made using reconstructed CT angiography images and categorized using scores of 0 to 3 based on hypothesized severity, giving a potential range of 0-38.
Results:We analyzed the CTA images on a cohort of 30 patients with acute (within 2 weeks of symptoms onset) type B aortic dissection who underwent TEVAR. The average age was 63 years (range 28-89 years) with 70% male and 50% Caucasian. The mean ASG score was 19 (range 10-29). We created an area under the receiver operating characteristic curve (AUROC) using ASG to predict aortic reinterventions. The area was 0.72 (95% CI 0.39 to 1.1). Guided by the AUROC, we divided patients into two groups, one with ASG scores <22 (n=20) and the other with scores >22 (n=10). With this cutoff, ASG exhibited 80% sensitivity and 76% specificity in predicting aortic reinterventions, with reintervention in 40% of high-score patients and 5% of low-score patients (P=0.031). In addition, patients in the high-score group were significantly younger (53.8 vs 66.9 years, P=0.006).
The mean thoracic aorta FLVI was 0.59 (range 0.19-0.94). Patients with high ASG score exhibited significantly larger thoracic aortic FLVI (0.73 vs 0.52, P=0.001). The correlation coefficient between thoracic aorta FLVI and ASG was 0.74 (P<0.001).
Conclusions:A preoperative ASG score of acute type B aortic dissections consists of analysis of the proximal landing zone, curvature and tortuosity of the aorta, dissection anatomy, aortic branch vessel anatomy, and supraceliac aorta anatomy. ASG score >22 correlated with larger false lumen to total aortic volume ratio and was an excellent predictor of aortic reinterventions.
Back to 2015 Annual Symposium Program
|






