Back to 2015 Annual Symposium Program
Sustained Hemodynamic Benefits Following Catheter Directed Interventions for Acute Pulmonary Embolism
Nathan L. Liang, MD, Rabih A. Chaer, MD, Luke K. Marone, MD, Michael J. Singh, MD, Michel S. Makaroun, MD, Efthymios D. Avgerinos, MD.
University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
OBJECTIVES:
Catheter-directed thrombolysis (CDI) for acute pulmonary embolism (PE) is commonly performed but hemodynamic benefits have not been clearly defined beyond the peri-procedural period. The objective of this study is to report midterm outcomes of CDI for treatment of acute PE.
METHODS:
Records of all patients who underwent CDI for massive (MPE) or submassive (SPE) pulmonary embolism were retrospectively reviewed. Endpoints were procedure-related complications, PE-related mortality, and longitudinal changes in echocardiographic parameters. Subgroup analysis was performed between MPE and SPE groups. Standard statistical techniques were used.
RESULTS:
69 patients underwent CDI for PE (mean age 59±15yrs, 56% male). 11 had MPE and 58 SPE. 21.7% had previous deep venous thrombosis (DVT) and PE; 52% had concurrent acute DVT. Troponin-I and BNP were abnormally elevated in 63% of patients. Baseline characteristics did not differ significantly by PE subtype.
52% of patients underwent ultrasound-assisted thrombolysis, 39% standard catheter-directed thrombolysis, and 8.7% aspiration, rheolytic therapy, or directed lytic bolus without continuous infusion. Bilateral interventions were performed in 89.9%. Average treatment time was 17.8±11.3h with average t-Pa dose of 24.2±14.6 mg.
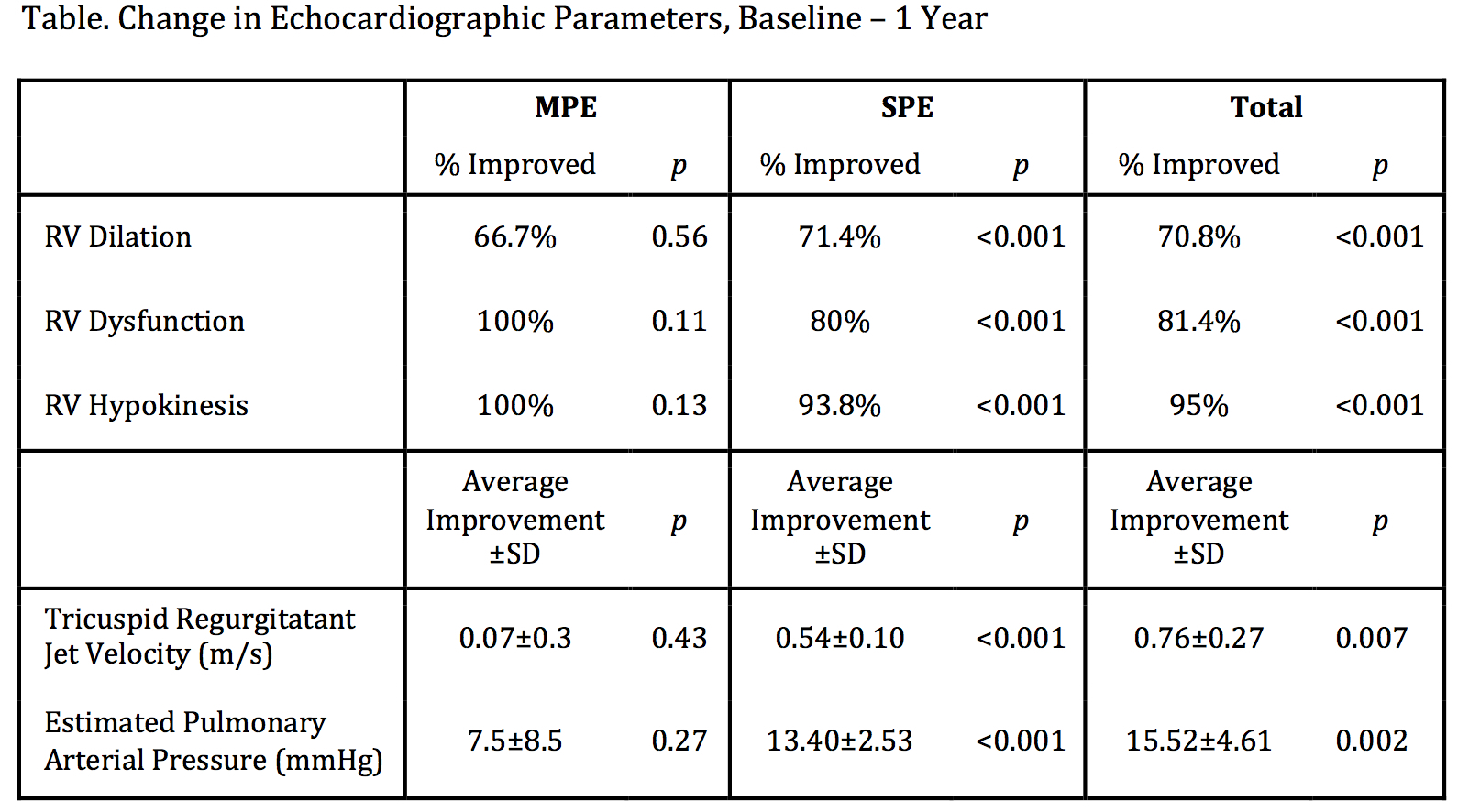
There was significant improvement in supplemental oxygen requirement in the cohort during hospitalization. There were 2 major (2.9%, requiring transfusion) and 6 minor (8.7%) peri-procedural bleeding complications with no strokes or cerebral hemorrhage. 3 patients (4.35%) required conversion to surgical thrombectomy. Significant improvement was demonstrated in all echocardiographic parameters between baseline and 1-year follow-up in the total cohort and in the SPE group; the MPE group improved in most parameters, but this was not statistically significant (Table). There was 1 PE-related death in each subgroup (9.1% MPE, 2.04% SPE, 3.3% overall), and all-cause mortality was 8.7% at 90 days. Survival at one year was 88%, and estimated survival by Kaplan-Meier analysis was 84.9±5.7% and 80.7±6.8% at 1 and 3 years.
CONCLUSIONS:
CDI are safe and effective for treatment of acute PE, with sustained hemodynamic improvement at one year. Further prospective large scale studies are needed to determine the comparative effectiveness of catheter directed intervention, systemic thrombolysis, and anticoagulation.
Back to 2015 Annual Symposium Program
|






