|
Back to 2015 Annual Symposium Program
What matters most in limiting amputations among diabetics: where you start, where you finish, or how much you improve?
Karina A. Newhall, MD1, Dan Gottlieb, MS2, Adrienne Faerber, PhD2, Emily Spangler, MD, MS1, Jonathan S. Skinner, PhD2, David Stone, MD1, Philip Goodney, MD, MS1.
1Dartmouth Hitchcock Medical Center, Lebanon, NH, USA, 2Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH, USA.
OBJECTIVE:
The risk of major leg amputation among patients with diabetes has declined over the past decade. This decline has coincided with increased focus on preventative measures for patients with diabetes, such as hemoglobin A1C monitoring and lipid testing. While many attribute the decline in amputations to improvements in the adoption of preventive measures, the relationship between the quality of diabetic care and amputation risk remains unclear.
METHODS:
We examined annual rates of hemoglobin A1C testing among all Medicare patients with diabetes between 2002 and 2012 across the 306 hospital referral regions (HRRs) defined in the Dartmouth Atlas of Healthcare. Within these regions, we examined annual rates of major leg amputation. We calculated correlation coefficients to examine the regional relationships between markers of diabetic care quality (annual hemoglobin A1C testing, lipid testing, and eye exams).
RESULTS:
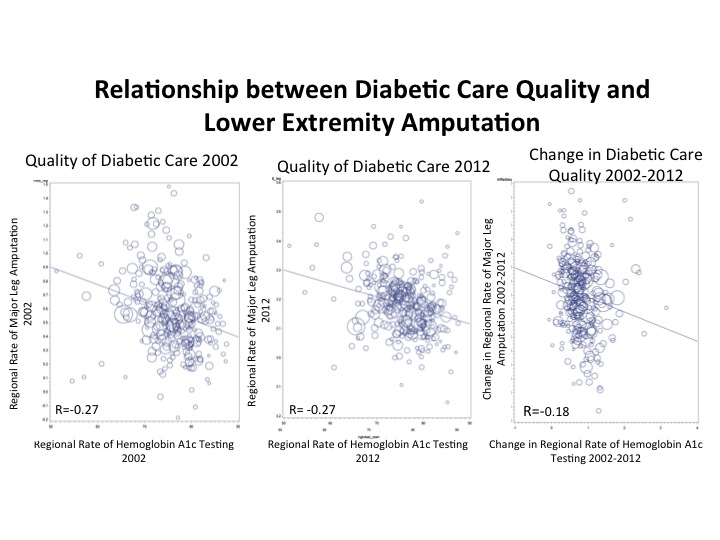
Overall, we found that 71% of diabetic patients had at least one hemoglobin A1c test, one blood lipid test, and one eye exam performed annually in 2002, and this proportion increased to 78% by 2012. Similarly, major leg amputation rate was approximately 4.4 per 1,000 among Medicare patients with diabetes in 2002, and decreased to 2.3 per 1,000 by 2012. When we compared relationships between regional-level hemoglobin A1C testing and amputation rate at start of our study period in 2002, at the end of our study in 2012, and by the rate of change during that time period, we found that high quality of diabetic care at the start and end of our study was more closely associated with lower amputation risk (R=0.27) than rapid improvement in the quality of diabetic care (R=0.18). Overall, none of these relationships were closely related to amputation risk (Figure).
CONCLUSION:
While improvements in the quality of diabetic care have occurred in recent years, these changes are not directly associated with a decline in amputation rate among Medicare patients with diabetes. Multifactorial studies examining the roles of specific preventive and therapeutic measures, not simply prevention, are needed to explain why amputation rates have improved for patients with diabetes.
Back to 2015 Annual Symposium Program
|






