Back to ePosters
Post-TEVAR Recurrent Type IB Endoleak: Treatment with Extension Cuffs and Endovascular Debranching
Nikita Tihonov, MD, Chad Jacobs, M.D., Bulent Arslan, MD, Gerard DeCastro, M.D., Walter McCarthy, M.D..
Rush University Medical Center, Chicago, IL, USA.
Post-TEVAR Recurrent Type IB Endoleak: Treatment with Extension Cuffs and Endovascular Debranching
Nikita Tihonov, MD, Gerard P. De Castro, MD, Chad E. Jacobs, MD, Walter J. McCarthy, MD
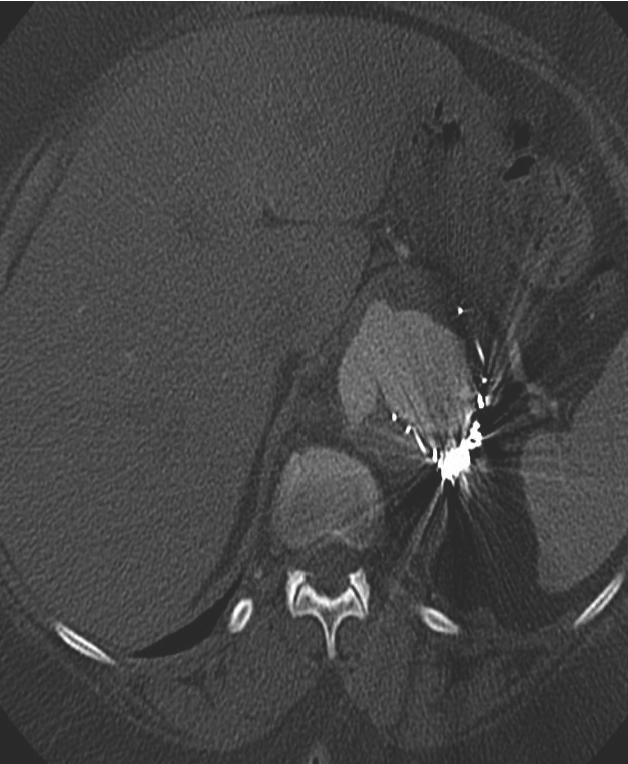
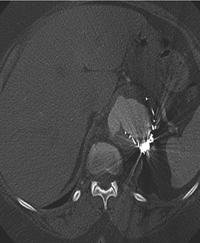
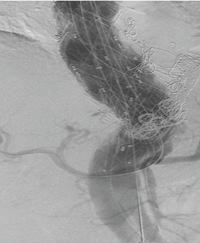
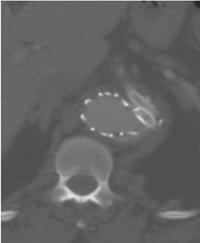
OBJECTIVE - The case involves redo-TEVAR with endovascular debranching of the celiac and SMA utilizing snorkel technique in a 72yo female with ESRD and recurrent type IB endoleak leading to enlargement of the aneurysmal component of the visceral segment aorta. Patient underwent TEVAR with Medtronic Talent stent graft in 2008 for treatment of a 6cm thoracic aortic aneurysm secondary to chronic type B aortic dissection. Endovascular cuff extensions and coil embolization were required for management of a type IB endoleak, which developed one year postoperatively. A recent CTA of the chest revealed a recurrent type IB endoleak with the increased diameter of the aneurysmal sac to 8cm. (Fig.1a,b).
METHODS - Redo-TEVAR and endovascular debranching was performed via bilateral femoral artery percutaneous access and a left axillary artery cutdown. The celiac and SMA arteries were preserved utilizing Viabahn and iCAST stents via snorkel technique from the left axillary artery access. A Medtronic Valiant Captivia endograft was deployed to cover the type IB endoleak and to bridge the previously placed Talent endograft. This was positioned 5mm below the uppermost edge of the visceral stents to maintain visceral perfusion.
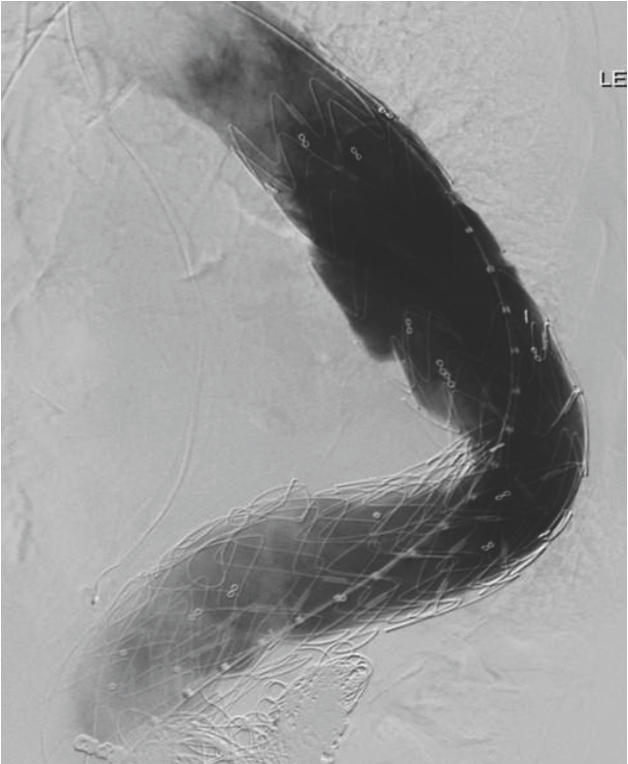
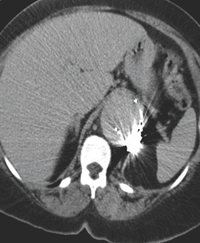
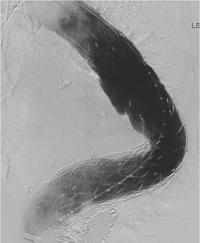
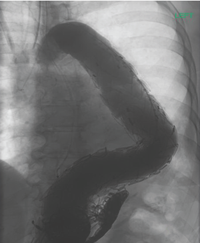
RESULTS - Completion arteriogram demonstrated successful placement of the Valiant endograft with excellent brisk flow into both the celiac and SMA. There was no evidence of the type Iendoleak. (Fig.1c). CTA two weeks post-procedure confirmed the absence of the type I endoleak and decreased size of the aneurysmal sac to 6.8cm.(Fig.1d).
CONCLUSION - Endoleak is a complication of endovascular management of AAA and TAA. Involvement of the endoleak at critical aortic branches, such as the visceral segment, can be particularly challenging. Hybrid treatment with distal aortic extension cuffs and open surgical visceral debranching has been described. This report illustrates an endovascular approach to redo-TEVAR using distal aortic endograft extensions with endovascular debranching via snorkel technique. This approach, using percutaneous femoral access for the extension cuffs and an axillary cutdown for the visceral snorkels, is a viable alternative in treating difficult endoleaks at critical aortic branches in selected cases.
Fig.1(a-f).
Back to ePosters
|