Back to 2016 Annual Symposium Abstacts
Cephalic Vein Transposition: A Durable Approach to Managing Cephalic Arch Stenosis?
Jon C. Henry, MD, Ulka Sachdev, MD, Michel S. Makaroun, MD, Steven A. Leers, MD.
University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
Objective: The proximal cephalic vein near the axillary vein (cephalic arch) is a common site of stenosis in patients with upper extremity arteriovenous fistulas for hemodialysis. Endovascular stenting of the stenosis and cephalic vein transposition to non-stenotic arm veins are two treatments employed. While both modalities have been reported in the literature as durable treatment options, there is a paucity of literature comparing the two. This study compares a large series of transpositions with endovascular treatment.
Methods: Patients with cephalic arch stenosis who underwent a cephalic vein transposition or endovascular procedures with stent deployment at the cephalic arch from January 1, 2008 to August 31, 2015 were obtained through a electronic record database search of one major medical center. Patients were excluded if the procedures were conducted outside of the system. A retrospective chart review of all patients was conducted to obtain: demographics, past medical history, procedural details, patency of the access, and the need for subsequent interventions.
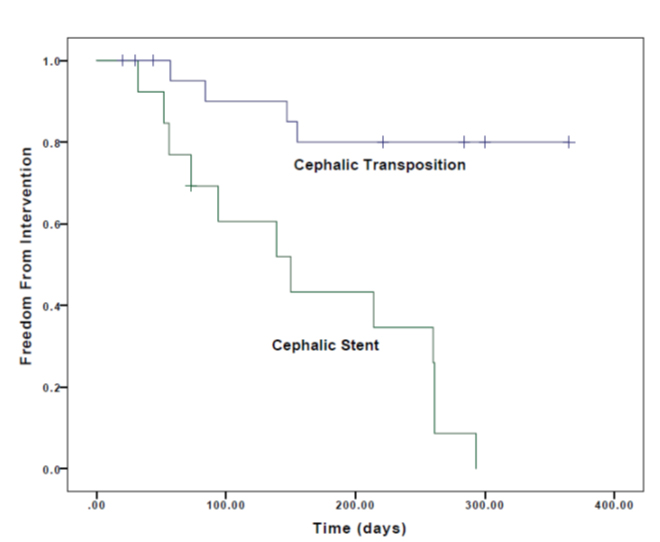
Results: Twenty-three patients underwent a cephalic vein transposition and thirteen patients had stenting of the cephalic arch. Patient demographics and past medical history were similar between the groups, but stenting procedures were more likely to be performed in younger accesses (1.55 years versus 2.99, p<0.001). Complications from the procedures were rare with only 2 hematomas in the transposition group and no documented complications in the stenting group (p = 0.525). At twelve months no patients were free from intervention in the stent group whereas 80% of the cephalic transposition patients were free from intervention (Figure 1, p<0.001). Overall access failure rate was similar between the two groups with overall patency of 70.7% in the cephalic transposition group and 51.3% of the stent group at four years (p=0.132).
Conclusions: Both cephalic vein transposition and cephalic arch stenting are successful at maintaining dialysis access with over half of the accesses remaining patent at four years. Cephalic vein transpositions are robust, require less follow-up re-interventions to maintain access patency, and should be the therapy of choice when feasible
Back to 2016 Annual Symposium Abstacts
|






