Back to 2016 Karmody Posters
Duplex Criteria for Renal Artery In-Stent Restenosis
Joseph Wuamett, MD, Michael Soult, MD, Sebastian Larion, MD, Sadie Ahanchi, MD, Jean Panneton, MD.
EVMS, Norfolk, VA, USA.
Objectives: The primary surveillance method to detect renal artery in-stent restenosis (ISR) is duplex ultrasound (DUS). The available literature suggests the velocity threshold for hemodynamically significant ISR (60-99%) is higher than in native renal arteries. However, there are no uniformly validated duplex criteria for ISR.
Methods: All patients that underwent renal artery stenting by a single vascular surgery group from 2008-2013 were retrospectively reviewed. A cohort of patients with repeat angiography and a paired pre-procedural renal duplex ultrasound was selected. Angiograms were analyzed to categorize 0-59% stenosis versus 60-99% stenosis. Mean peak systolic velocity (PSV), mean end diastolic velocity (EDV), and mean renal artery aorta ratio (RAR) for renal arteries were collected from DUS exams performed within 6 months of angiogram. The full spectrum of data was analyzed with receiver operator characteristics curve analysis (ROC) to determine the cutoff PSV, EDV, and RAR for ISR. Cutoff values for ISR were chosen to maximize the sensitivity and specificity.
Results: A total of 257 renal artery stents were reviewed, yielding 128 renal artery stents with acceptable angiograms (112 catheter based, 16 computed tomography) and paired renal DUS. Angiography demonstrated 60 renal artery stents with <60% stenosis and 68 renal artery stents with >60% stenosis. Mean PSV, EDV, and RAR for <60% renal ISR versus >60% renal ISR were as follows: 182 cm/s vs. 418 cm/s (p<0.001), 36 cm/s vs. 105 cm/s (p<0.001), and 2.79 vs. 5.9 (p<0.001), respectively. Areas under the operator curve for PSV, EDV, and RAR were 0.95, 0.89, and 0.89, respectively. The cutoff PSV, EDV, and RAR values for >60% renal ISR were 254.5 cm/s (sensitivity: 95.59%, specificity: 83.33%), 55.05 cm/s (sensitivity: 79.69%; specificity: 87.73%), and 3.05 (sensitivity: 93.65%; specificity: 70.21%), respectively.
Conclusions: Renal artery duplex is a reliable surveillance tool for detecting hemodynamically significant renal artery ISR with PSV, EDV, and RAR thresholds that are higher than in the native renal artery. A PSV >254.5 cm/s appears to be the most useful criteria for distinguishing ISR. This large series adds to a growing body of literature suggesting vascular laboratories adjust duplex criteria when monitoring renal artery stent patency. 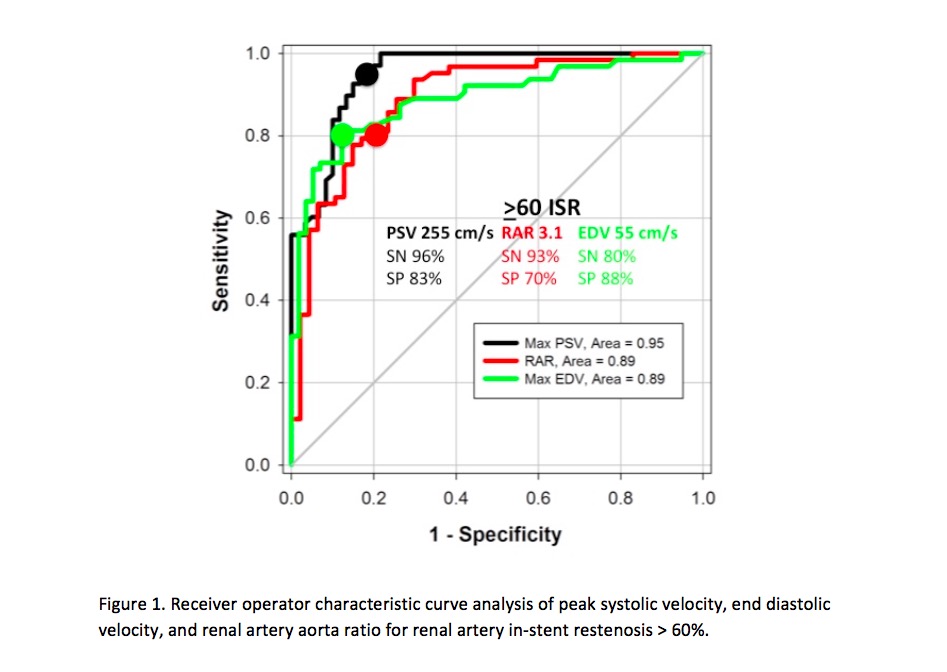
Back to 2016 Karmody Posters
|






