Back to 2016 Karmody Posters
Underutilization of Antiplatelet and Statin Therapy following Postoperative Myocardial Infarction within the Vascular Quality Initiative
Andrea M. Steely1, Peter W. Callas2, Randall R. De Martino3, Patrick K. Hohl1, David J. Schneider1, Daniel J. Bertges1.
1The University of Vermont Medical Center, Burlington, VT, USA, 2The University of Vermont College of Medicine, Burlington, VT, USA, 3Mayo Clinic, Rochester, MN, USA.
OBJECTIVE: To investigate adherence to practice guidelines for cardiac medication (CM) use after postoperative myocardial infarction (POMI) following vascular surgery in a multicenter registry.
METHODS: CM use was examined in 2,042 patients with POMI following vascular surgery within the Vascular Quality Initiative (VQI). Our primary aim was to assess CM use after POMI, defined as (1) single (aspirin or P2Y12 antagonist) antiplatelet (SAPT) or dual (aspirin and P2Y12 antagonist) antiplatelet therapy (DAPT) and (2) statin therapy at discharge. Our secondary aim was to analyze long term mortality following surgery based on CM. A third aim was to evaluate regional differences in CM utilization after POMI.
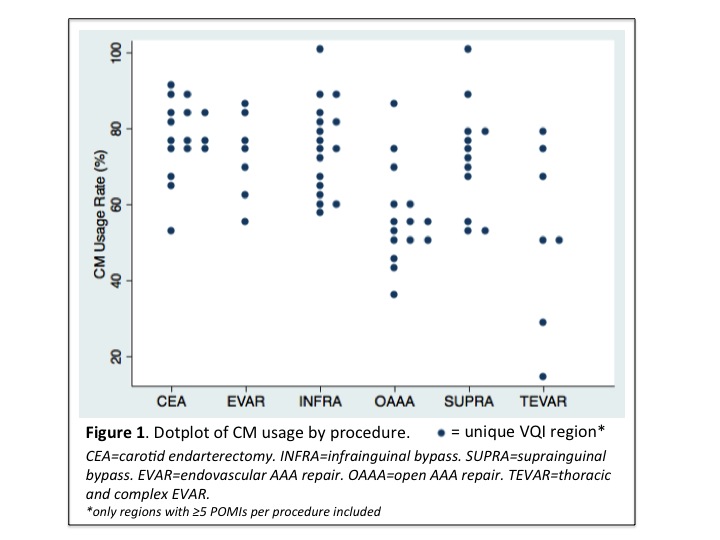
RESULTS: Overall CM use after POMI included SAPT (50%), DAPT (34%), and statin therapy (75%). 29% of patients with POMI were not receiving combined antiplatelet and statin therapy at discharge. For patients discharged on combination therapy, SAPT (41%) was more common than DAPT (30%). Patients with POMI undergoing carotid endarterectomy were more likely to be discharged on CM (80%) compared to thoracic endovascular aneurysm repair (56%), open abdominal aortic aneurysm repair (AAA) (58%), endovascular AAA repair (69%), suprainguinal bypass (71%), and infrainguinal bypass (77%) (P<.001). Regional variation in CM prescription at discharge following POMI was also observed with a range of 14%-100% (P=.03) (Fig 1). Patients with POMI not discharged on CM after POMI had higher rates of late mortality compared to those on antiplatelet and statin (log rank P<.001), with mortality rates of 60% and 24% at mean of 570 days, respectively.
CONCLUSIONS: Within the VQI, regional and procedure-specific variation exists in CM regimen after POMI following vascular surgery. Absence of combined antiplatelet and statin therapy at discharge after POMI was associated with higher late mortality and represents an area for quality improvement in the care of these patients.
Back to 2016 Karmody Posters
|






