|
Back to 2016 Annual Symposium Abstacts
Aortic Curvature as a Predictor of Intraoperative Type IA Endoleak
Richte C.L. Schuurmann1, Kenneth Ouriel2, Bart E. Muhs3, William D. Jordan, Jr.4, Richard Ouriel2, Johannes T. Boersen1, Jean-Paul P.M. De Vries1.
1St. Antonius Hospital, Nieuwegein, Netherlands, 2Syntactx, New York, NY, USA, 3Yale School of Medicine, New Haven, CT, USA, 4University of Alabama, Birmingham, AL, USA.
Objective: Hostile neck characteristics are associated with complications such as type IA endoleak after endovascular aortic repair (EVAR). Aortic neck angulation is one such characteristic, but its association with complications has not been uniform between studies. Neck angulation assumes triangular oversimplification of the aortic trajectory, which may explain conflicting findings. By contrast, aortic curvature describes the actual trajectory and may provide better predictive value for neck complications.
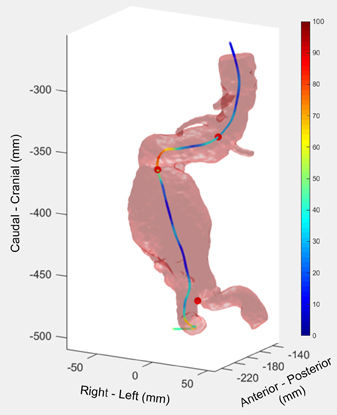
Methods: Data was retrieved from the Heli-FX Aortic Securement System Global Registry (ANCHOR). One cohort included patients who presented with intraoperative endoleak type IA at completion angiogram and a second cohort comprised those without intraoperative or late type IA endoleak. The aortic trajectory was divided into six segments with potentially different influence on the stent graft performance: suprarenal, juxtarenal and infrarenal aortic neck (-30 to -10, -10 to 10 and 10 to 30 mm from lowest renal artery, respectively), the entire aortic neck, aneurysm sac and terminal aorta (20 mm above bifurcation to bifurcation). Curvature was automatically calculated over the six segments by numerical computation. Aortic curvature was compared to other standard neck characteristics including neck length, neck diameter, maximum aneurysm sac diameter, neck thrombus and calcium, suprarenal and infrarenal angulation and neck tortuosity index. Independent risk factors for intraoperative type IA endoleak were identified using backwards stepwise logistic regression. For the variables in the final regression model, suitable cutoff values in relation to prediction of acute type IA endoleak were defined with the region under the ROC curve.
Results: The analysis included 64 patients with intraoperative type IA endoleak and 79 controls. Logistic regression identified only aortic neck calcification and aortic curvature, expressed over the juxtarenal aortic neck, the aneurysm sac and the terminal aorta, as independent predictors of intraoperative type IA endoleak.
Conclusion: Neck calcification and aortic curvature, expressed within the juxtarenal aortic neck, aneurysm sac and terminal aorta, appear to be the best predictors of intraoperative type IA endoleak. Aortic neck angulation was not a predictor for acute failure. Aortic curvature may provide a better anatomic characteristic to define patients at risk for early complications after EVAR.
Back to 2016 Annual Symposium Abstacts
|






