Back to 2016 Annual Symposium ePosters
A Systematic Approach to the Management of Patients with Disseminated Mycotic Aneurysms Post Intravesicular BCG Treatment for Bladder Cancer
Anahita Dua, MD, MS, MBA, Daniel Davila, MD, Brian Keyashian, MD, Shahriar Alizadegan, MD, Gary Seabrook, MD, Kellie Brown, MD, Brian Lewis, MD, Michael Malinowski, MD, Cheong J. Lee, MD.
Medical College of Wisconsin, Milwaukee, WI, USA.
OBJECTIVES:
BCG is a well-accepted treatment for bladder cancer. Case reports have detailed the relationship between instillations and development of disseminated aneurysmal disease. Few studies have discussed the systematic approach to such patients. Delay in diagnosis/treatment results in patients presenting with aneurysm rupture. This reports aims to discuss the workup and management of patients with aneurysms resulting from disseminated mycobacterium after BCG instillations for cancer.
METHODS:
A 63-year-old male patient was diagnosed with bladder carcinoma in 2012 which was treated with resection and intravesical instillations of BCG. In 2015 he presented to the ED with a ruptured popliteal aneurysm. CTA revealed a popliteal aneurysm in the other leg, bilateral common femoral aneurysms and a right common iliac aneurysm. The popliteal aneuryms were repaired with stenting and the femoral aneurysms repaired
with Dacron interposition grafts. The iliac aneurysm was repaired endovascularily. The patient had an unintentional 80-pound weight loss and intermittent nocturnal fevers and chills that had persisted for over an 8 month period. Malabsorptive and malignancy workup revealed no etiology but the final pathology from the femoral aneurysm sac reported Mycobacterium bovis within the wall of the artery. He was started on
anti-tuberculosis therapy (ethambutol, isoniazid, rifampin), nutritional
support via TPN and underwent close CTA surveillance.
RESULTS:
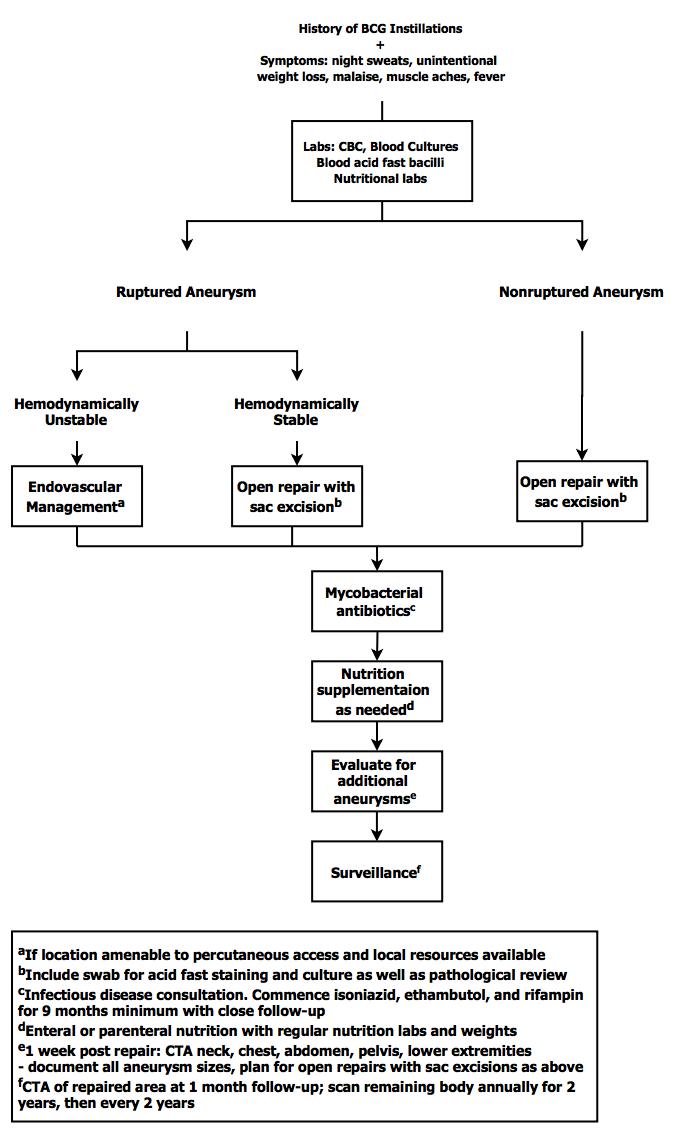
Based on our experience with this patient, an algorithm was devised to approach patients who have a history of BCG bladder instillations (Figure I).
CONCLUSIONS:
A thorough history in conjunction with anti-tuberculosis treatment and surgical excision of aneurysmal tissue is the cornerstone of therapy in patients who develop mycotic aneurysms from BCG instillations. Patients should also be closely monitored for new aneurysms which should be repaired electively in an open fashion.
Back to 2016 Annual Symposium ePosters
|






