
Multi-Institution Review of Limited Aortic Graft Infections Treated with Obturator and Hemi-NAIS Bypass
Jonathan Bath1, Matthew R. Abate2, Maham R. Rahimi1, Michael C. Scott2, Becky Long3, Efthymios Avgerinos3, Joseph Giglia1, Ahsan T. Ali2, Matthew R. Smeds2.
1University of Cincinnati, Cincinnati, OH, USA, 2University of Arkansas for Medical Sciences, Little Rock, AR, USA, 3University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
OBJECTIVES: Infections of isolated limbs of prosthetic grafts are challenging. Management can be morbid, involving removal of part or of all prosthetic material and aortic reconstruction. More limited resections of only infected material and reconstruction of the affected iliac may be possible. We review two academic institution experiences treating limited aortic graft infections by obturator canal bypass (OCB) or hemi-neoaortoiliac system (H-NAIS).
METHODS: Retrospective review of OCB at one institution between 1995 and 2013 and H-NAIS at the other institution between 2003 and 2014 was conducted. Demographics, co-morbidities, post-operative and medium-term events were recorded. Outcomes were patency, limb salvage and survival.
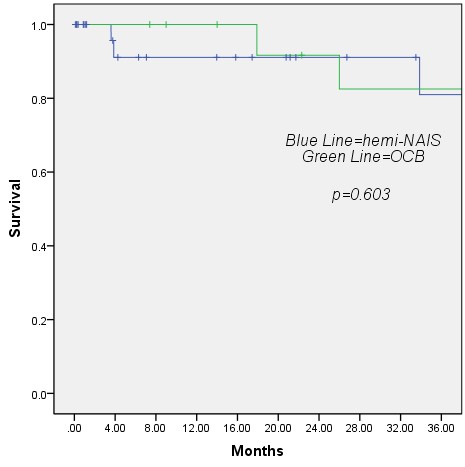
RESULTS: OCB was performed in 18 limbs and H-NAIS in 34 limbs. OCB group had a higher prevalence of cancer (40% vs. 10%; p=0.04). The commonest treatment indication was infection of an aortobifemoral bypass limb in both groups. No differences in overall superficial wound infection were seen (6% in OCB versus 3% in H-NAIS respectively; p=1.00) nor overall persistent graft infection (6% of OCB versus 0% in H-NAIS; p=0.35). The most frequent organism cultured in both OCB and H-NAIS was S. Aureus. Surgery duration was similar between OCB and H-NAIS (380 vs. 370 minutes; p=0.8) as was length of stay (12.4 vs. 10.4 days; p=0.4). At 24 months there was no difference in primary patency between groups (OCB 65% vs. H-NAIS 63%; p=0.7), primary-assisted patency (OCB 71% vs. H-NAIS 69%; p=0.5) or secondary patency (OCB 71% vs. H-NAIS 88%; p=0.6). Endovascular (44% vs. 18%; p=0.03) and open (61% vs. 32%; p=0.04) reinterventions occurred more frequently in OCB than H-NAIS. There were no differences in overall survival (OCB 83% vs. H-NAIS 81% ;p=0.6) (Figure 1) or limb salvage (OCB 81% vs. H-NAIS 74%; p=0.8) at 36 months .
CONCLUSIONS: OCB and H-NAIS may be effective strategies for treatment of limited aortic graft infections with reasonable patency, survival and limb salvage at medium-term follow-up. Prudent patient selection and institutional experience with aortic graft infection treatment leads to good medium-term outcomes with lifelong follow-up recommended. Further study of the optimal treatment strategy for this complex group of patients is needed.
Back to 2017 ePosters



