
The Simultaneous Neointimal Fibroplasia (NIF) of the Common Femoral Arteries, a Case Report
David Dockray, MD, Anthony J. Comerota, MD.
ProMedica Toledo Hospital, Toledo, OH, USA.
Objective: To report the rapid simultaneous development of pre-occlusive neointimal fibroplasia 10 months following simultaneous bilateral common femoral artery endarterectomy.
Methods: A 58 year-old caucasian female underwent aortic stenting, bilateral common and external iliac artery stenting and bilateral common femoral artery endarterectomy for lifestyle limiting intermittent claudication (IC). Her ABIs were 0.6 bilaterally.
She enjoyed transient improvement in her capacity to ambulate. Her walking distance began to diminish within 4 months and by 10 months postop she had disabling IC bilaterally and nocturnal ischemic rest pain in her left foot. ABIs were 0.55 on the right and 0.45 on the left with minimal pulsatile perfusion to the right foot and no pulsatile profusion to the left foot.
CTA showed a patent aorta and iliac stents bilaterally, with pre occlusive stenoses of both CFAs.
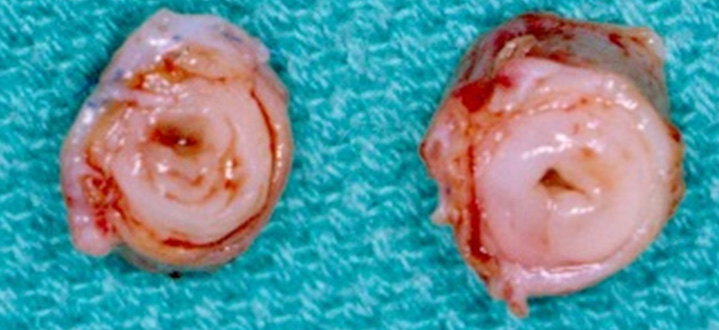
The patient underwent resection of both CFAs, which had pre-occlusive neointimal fibroplasia (Figure 1), a reconstruction with 8 mm ringed heparin bonded PTFE grafts. Both proximal anastomoses were to the stented EIAs. The distal anastomoses were end-to-end to the right SFA with re-implantation of the profunda femorus artery into the graft and a left end-to-end anastomosis to the profunda femorus artery.
Results: Post-operative ABIs were 1.0 on the right and 0.65 on the left with good pulsatile perfusion to both feet. The right leg was asymptomatic and the left leg had long-distance tolerable IC. At one year follow-up the patient's left IC is nearly resolved. Microscopic analysis was consistent with neointimal fibroplasia.
Conclusions: The simultatneous CFA endarterectomy led to rapid simultaneous development of NIF to pre-occlusive lesions. It appears the same artery will develop NIF at the same rate of proliferation if intervention is similarly performed. What remains to be answered is whether a different artery has the same biologic potential to develop the NIF from a similar intervention. This case illustrates an intriguing observation having implications for patient care.
Back to 2017 ePosters



