
Staged Hybrid Repair of a Large Congenital Renal Arteriovenous Fistula
Patric Liang, MD, Mark Wyers, MD.
Beth Israel Deaconess Medical Center, Boston, MA, USA.
OBJECTIVES: Congenital renal arteriovenous fistulas (CRAVFs) are rare lesions that can lead to hematuria, hypertension, heart failure, and rupture. Percutaneous arterial embolization is used in selected patients with small renal CRAVFs, with safe and effective outcomes. However, concerns remain for percutaneous treatment of large, high-flow CRAVFs, which may lead to paradoxical embolization and require ongoing long-term follow-up. We describe a staged procedure that combines both endovascular embolization and open resection to treat large CRAVFs with preservation of renal parenchyma. METHODS:
Using hospital inpatient and outpatient records, we identified one patient with a large CRAVF. We reviewed the patient's presentation, our surgical technique, and 2-year outcome from the intervention. Clinical success was evaluated by technical feasibility, renal parenchymal preservation, re-intervention, and freedom from recurrence. RESULTS:
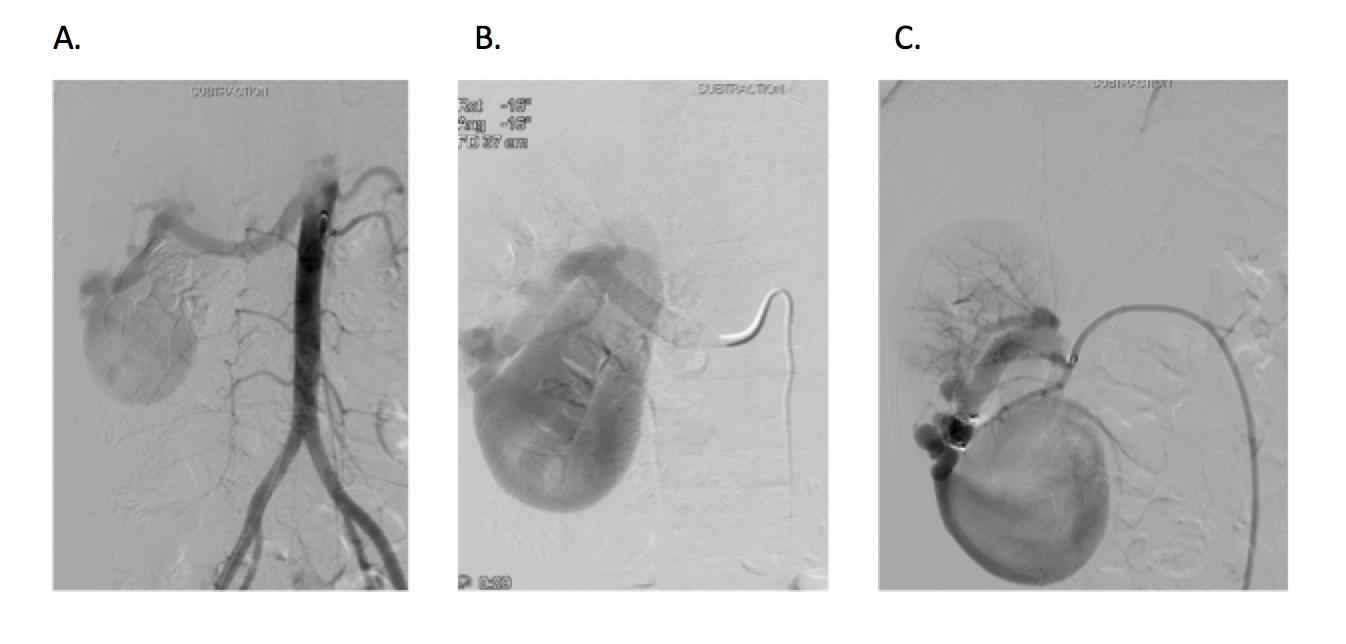
A 35 year-old female was noted to have a harsh back bruit on physical exam. A large 9x4x4cm CRAVF was identified at the right renal hilum on noninvasive imaging, partially compressing the renal pelvis and causing right-sided hydronephrosis. Diagnostic abdominal angiogram revealed a large arterial branch feeding into the CRAVF and a large exophytic venous aneurysm component. The CRAVF was repaired in two stages. Percutaneous Amplatzer embolization of the arterial inflow was first performed (Figure 1), followed two days later by open resection of the venous aneurysm component with primary repair of the right renal vein. Pretreatment of the arterial inflow greatly simplified the open procedure by depressurizing the CRAVF and eliminating the need for formal inflow control. Patient was discharged home on post-operative day 3. No re-interventions were needed during 2-year follow-up. 3-month and 2-year interval computed tomography angiography scans showed complete preservation of the right kidney with no recurrence or residual CRAVF. CONCLUSIONS:
Percutaneous arterial embolization of large renal CRAVFs can lead to central embolization from residual venous thrombosis. The safety of repairing large renal CRAVFs is greatly enhanced by this hybrid approach and does not require subsequent long-term follow-up. Figure 1. (A) Abdominal angiogram showing rapid filling into a large CRAVF at the inferior pole of the right kidney. (B, C) Selective catheterization and embolization of the feeding artery.
Back to 2017 ePosters



