
Novel Adjunct Technique to Facilitate Proximal Aortic Arch Extension During TEVAR for Chronic Type B Aortic Dissection
Clayton Brinster, MD, Taylor Smith, MD, Hernan Bazan, MD, W C. Sternbergh, MD.
Ochsner Clinic Foundation, New Orleans, LA, USA.
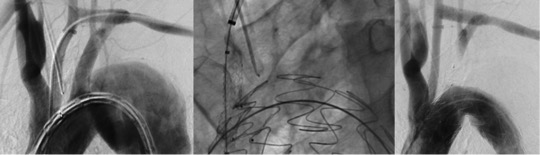
OBJECTIVES: Proximal landing zone extension into the aortic arch is frequently required during TEVAR to effectively treat chronic type B aortic dissection (CTBAD). However, complex arch anatomy can make proximal seal challenging. We report a unique approach to assist in proximal extension during TEVAR in the treatment of CTBAD. METHODS: A database at a single institution was examined to identify cases in which a staged left carotid-subclavian bypass was accessed to facilitate proximal landing zone extension into the aortic arch during TEVAR for CTBAD. RESULTS: Between 2011 and 2016, 88 patients underwent TEVAR. In four patients, a left carotid-subclavian bypass was accessed from a brachial approach to facilitate proximal landing zone extension to treat CTBAD. All four patients were men and the average age was 54 (43 to 67). The average maximal thoracic aortic diameter was 64mm (51 to 85) and the average interval from dissection to TEVAR was 35 months (3 to 120). Extension to cover Zone I of the aortic arch was achieved in two patients in which the bypass was accessed to place a left common carotid artery "chimney" stent at the time of TEVAR (Figure). In similar fashion, the bypass was utilized to access the true lumen in two patients with complex proximal dissection flaps, allowing Zone II coverage after a wire from the bypass was snared from a femoral approach. Technical success was achieved in all patients. There were no postoperative neurologic events. After an average follow-up of 21 months (6 to 26), false lumen thrombosis and aortic diameter regression were observed in all patients. CONCLUSIONS: We report, for the first time, the use of a staged carotid-subclavian bypass to facilitate accurate extension into Zones I and II of the aortic arch during TEVAR for CTBAD. In well-defined cases, this technique may obviate the need for surgical exposure of the left common carotid artery for retrograde stent placement or for extended surgical debranching when Zone I coverage is required. In addition, this approach allows reliable delineation of complex distal arch anatomy and access to the true lumen when attempts from a femoral approach are unsuccessful.
Back to 2017 ePosters



