
Limb Occlusion as a Manifestation of Endologix Graft Failure
Marvin E. Morris, MD, Heepeel Chang, MD, Matthew D. Kronick, MD, Marc Norris, MD, Neal C. Hadro, MD.
Baystate Medical Center, Springfield, MA, USA.
Introduction: Component separation leading to type III endoleak of the Endologix AAA device is an evolving clinical problem. Recent literature has provided insight to mechanisms of type III failure this device. We provide a case series suggesting that limb occlusion may reflect morphological AAA changes leading to type III component separation and failure. Additionally, smaller aneurysm (5cm) can also succumb to the component separation failure. Methods: A two-year retrospective review of patients treated for type III endoleaks after Endologix AAA graft placement. For our analysis, we compared the initial AAA neck diameter, maximal AAA size during initial implant, length of aortic coverage, extent of overlap of device pieces and time to treatment failure. Results: A total of 5 patients required intervention for type III endoleak. The clinical presentation included rupture preceded by limb occlusion (1), acute limb ischemia requiring surgical thrombectomy (1), the remaining were detected on serial surveillance imaging (3) with an increase in AAA diameter. Anatomical and technical details are as follow: Mean aortic neck diameter 24.5mm, mean maximal AAA diameter 5.4cm, mean aortic coverage length 96cm, mean extent of overlap 5.9cm. Time to treatment failure ranged from 1.6 to 5.4 years. Type III endoleaks were treated by relining the with new AFX device in 2 patients, or AFX cuffs (2) with a Palmaz stent in 3 patients. Conclusion: Type III endoleaks following Endologix AAA device implantation is an evolving problem. A limb occlusion after AFX deployment could suggest a change in the morphology of the AAA-EVAR complex and a potential harbinger of potential rupture. We have identified small AAA, mean 5.4cm in our series, and may also have a type III device failure. Diligent follow up is requisite to identify patients at risk for type III endoleak formation after early generation Endologix graft deployment.
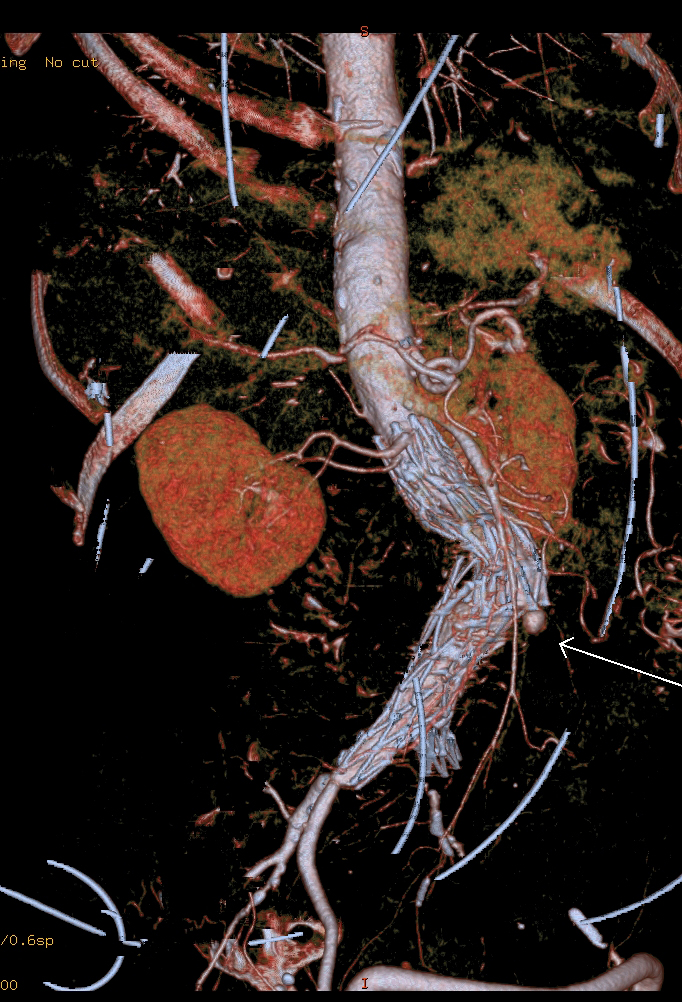
Figure 1: Significantly deformed AFX with clear separation of the components, note femoral-to-femoral bypass for previous limb occlusion. Post-repair image with (2) 28mm Aortic cuffs and Palmaz stent.

Back to 2017 ePosters



