
Impact of Cardiac Cycle on Thoracic Aortic Geometry and Assessment of Aortic Strain and Distensibility-A Computed Tomography Morphometric Analysis
Muhammad M. Zubair, MD, Hector de Beaufort, MD, Adeline Schwein, MD, Eric Y. Yang, MD, Luis F. Gomez, MD, Ahmed Mohamed, MD, Ali Irshad, MD, Faisal Nabi, MD, Carlos F. Bechara, MD, Ponraj Chinna Durai, MD, Jean Bismuth, MD.
Houston Methodist Hospital, Houston, TX, USA.
OBJECTIVES: Understanding morphological changes of the thoracic aorta with cardiac motion is critical for TEVAR planning. The aim of this study was to assess morphometric changes with cardiac cycle and quantify arterial strain and distensibility in a group of patients being evaluated for trans-aortic valve replacement (TAVR). METHODS: I n this retrospective study, EKG-gated cardiac CT from 116 patients who were evaluated for TAVR were reviewed. A protocol for measurements of maximal diameters and lengths of the thoracic aorta was established (Figure 1). End-systolic and end-diastolic cardiac CT phases were defined by assessing the lowest and highest left ventricular volumes respectively. Measurements were made in multi-planar views perpendicular to the semi-automatically created centerline on both systolic and diastolic phases, using a commercially available software Syngo.Via (Siemens Healthcare GmbH, Germany). Aortic strain and distensibility at various aortic levels were calculated according to accepted definitions. RESULTS: Mean age was 77±11 years. Mean systolic and diastolic diameter was 31.6±0.42 and 30.1±4.4 mm at the sinotubular junction (STJ; location 1), 35.6±4.8 and 34.8±4.7 mm in the ascending aorta (location 2), 29.1±3.3 and 28.5±3.3 mm in the aortic arch (location 6), and 26.7±5.4 and 25.8±5.4 mm in the descending aorta (location 9). Mean diameter change was 1.5±0.9 mm at the STJ, 0.8±0.9 mm in the ascending aorta, 0.6±0.8 mm in the aortic arch, and 0.9±1.2 mm in the descending aorta. Mean arterial strain and distensibility were 5.0±3.2% and 1.2±0.9 %/kPa-1 at the level of the STJ, 2.4±2.7% and 0.6±0.7 %/kPa-1 in the ascending aorta, 2.0±2.9% and 0.5±0.7 %/kPa-1 in the aortic arch, and 3.9±5.7% and 1.0±1.8 %/kPa-1 in the descending aorta. On univariable analysis, there was a significant negative correlation between distensibility in the aortic arch and BMI (Spearman’s rho -0.2, p=0.027), while differences in distensibility across age, gender, or race were not significant at any of the locations in the thoracic aorta. CONCLUSIONS: In a cohort of patients under evaluation for TAVR, average values of aortic strain and distensibility in the thoracic aorta were small. Distensibility was related to BMI but not to gender, race or age. These findings may have implications for TEVAR planning. 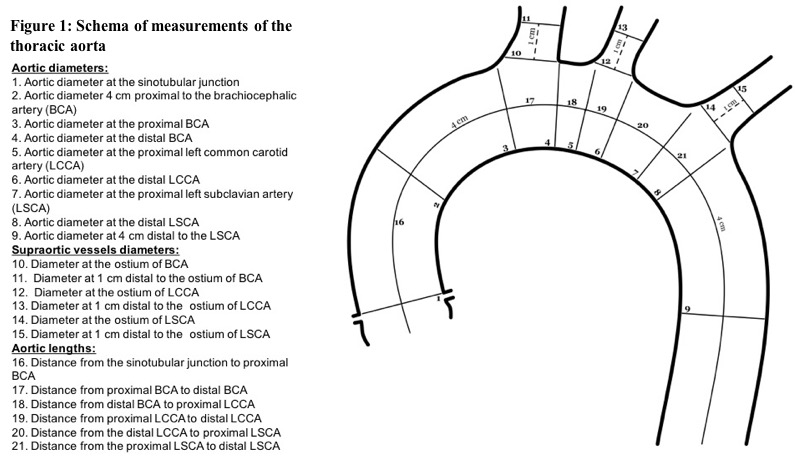
Back to 2018 ePosters



