
Complete vs. Partial Excision of Infected Arteriovenous Grafts: Does Remnant Graft Material Impact Outcomes?
Rui Han Liu, BS, Charles D. Fraser, III, MD, Xun Zhou, MD, Robert J. Beaulieu, MD, Thomas Reifsnyder, MD.
The Johns Hopkins Hospital, Baltimore, MD, USA.
OBJECTIVES: Infected arteriovenous grafts necessitate intervention to obtain source control. However, excising graft material can be challenging and may lead to complications. Leaving a cuff of graft at the sites of anastomosis allows for avoidance of potential risks, but it is unclear if doing so places patients at risk for recurrent graft infection. The purpose of this study is to investigate the impact of complete versus partial excision of infected arteriovenous prosthetic dialysis access.
METHODS: All patients who underwent surgical intervention for infected arteriovenous grafts at a single institution were retrospectively reviewed. Patients were grouped according to intervention type: complete excision and partial excision of arteriovenous prosthetic grafts. Primary outcome was freedom from subsequent intervention for infection, defined as number of days from excision to subsequent reoperation for reinfection. Freedom from infection was analyzed using the Kaplan Meier method.
RESULTS: 111 patients underwent surgical intervention for infected arteriovenous grafts from 2003 to 2016. 63.1% (n=70) underwent partial excision of infected arteriovenous grafts. The remainder (37%, n=41) underwent complete excision with vascular repair. Median follow up time was 906 days (IQR:198-1619). The most common causative organisms included methicillin resistant Staphylococcus aureus (n=32, 28.8%), methicillin sensitive Staphylococcus aureus (n=15, 13.5%), vancomycin resistant Enterococcus (n=4, 3.6%), and Staphylococcus epidermidis (n=4, 3.6%). The recurrent infection rate in the partial excision group was 12.9% (n=9) compared with 2.44% (n=1) in the complete excision group (p=0.064). 11.4% (n=8) of patients in the partial excision group required reoperation for recurrent infection compared to none in the complete excision group (p=0.025). 1 patient undergoing complete excision developed postoperative aneurysm requiring reoperation while another undergoing complete excision required exploration for bleeding.
CONCLUSIONS: Incomplete excision of infected arteriovenous prosthetic grafts may be associated with a higher rate of reinfection when compared to complete graft excision. Although rates of recurrent infection did not reach statistical significance, rates of postoperative infection requiring reoperation were statistically different between these groups. Complete excision presents technical challenges but may provide superior source control in managing infected dialysis access. Complete excision with vascular reconstruction should be performed when possible to avoid leaving remnant prosthetic material. 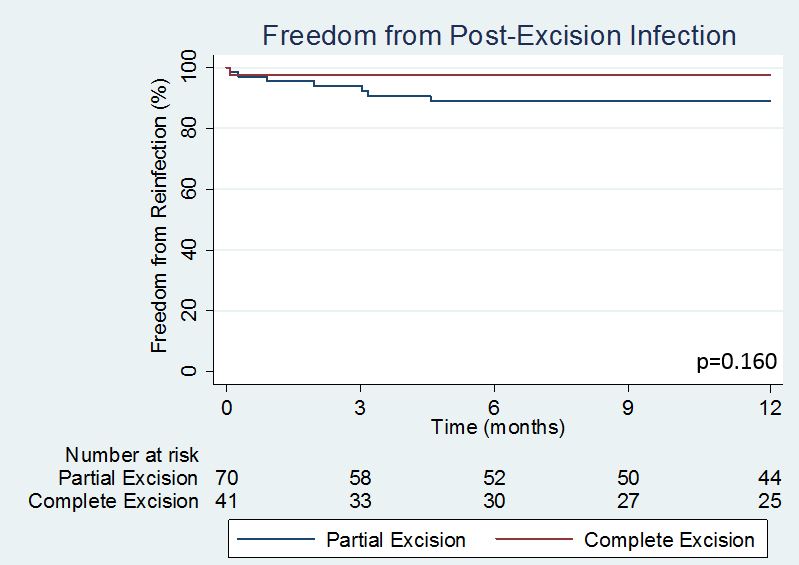
Back to 2018 Program



