
Impact of Patient Safety Indicators on Readmission Following Abdominal Aortic Surgery
Jonathan Bath1, Viktor Y. Dombrovskiy2, Todd R. Vogel1.
1University of Missouri, Columbia, MO, USA, 2UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ, USA.
OBJECTIVES: Patient safety is critical for health care quality and measures created by the Agency for Healthcare Research and Quality (AHRQ) identify hospitalizations with potentially preventable adverse events. This analysis evaluated whether Patient Safety Indicator events (PSI) following open abdominal aortic aneurysm (AAA) or endovascular abdominal aortic repair (EVAR) increased readmission risk.
METHODS: Patients undergoing elective repair of non-ruptured AAA (2009-2012) in Medicare Provider Analysis and Review (MedPAR) were selected using ICD-9-CM codes. To identify PSI events, we utilized the AHRQ Patient Safety Indicator ICD-9-CM numerator codes. Chi-square analysis and logistic regression models were created to predict the likelihood of 30-day readmission adjusting for age, sex, gender, hospital factors, comorbidities and the occurrence of safety events.
RESULTS: 66,923 patients undergoing elective AAA repair were evaluated: Open (9,315) and EVAR (57,608). The overall 30-day readmission rate was 10.5%. The occurrence of a PSI event was 1.83 more likely to lead to a 30-day readmission compared with no event (CI, 1.69 -1.96). Frequent PSI events after open vs. EVAR were: PSI 11 postoperative respiratory failure (17.7% vs. 1.8%, p<.0001); PSI 9 perioperative hemorrhage (3.6% vs. 2.6%, p<.0001); PSI 13 postoperative sepsis (3.5% vs. 0.4%, p<.0001); PSI 15 accidental puncture or laceration (2.1% vs. 0.6%, p<.0001); and PSI 10 postoperative acute kidney injury requiring dialysis (1.4% vs. 0.2%, p<.0001). Odds of 30-day readmission were 66% higher for postoperative acute kidney injury requiring dialysis (CI, 1.28-2.15), 36% higher for postoperative respiratory failure (CI, 1.22-1.52), 34% higher for perioperative hemorrhage (CI, 1.18- 1.52), and 126% higher for postoperative pressure ulcer (CI, 1.68-3.05). Occurrence of any PSI event was associated with an increased length of stay, intensive care days, and charges (all p<0.001). Readmission at 30 days (Figure 1) was significantly higher if any PSI event occurred (p<0.0001).
CONCLUSIONS: The odds of 30-day readmission after AAA surgery were 83% higher when a PSI event occurred. Minimizing preventable PSI events would decrease hospital utilization and decrease the likelihood of 30-day readmission after open and endovascular AAA repair. PSI events may be used to identify patients at greatest risk for readmission and offer opportunities to lower future readmissions 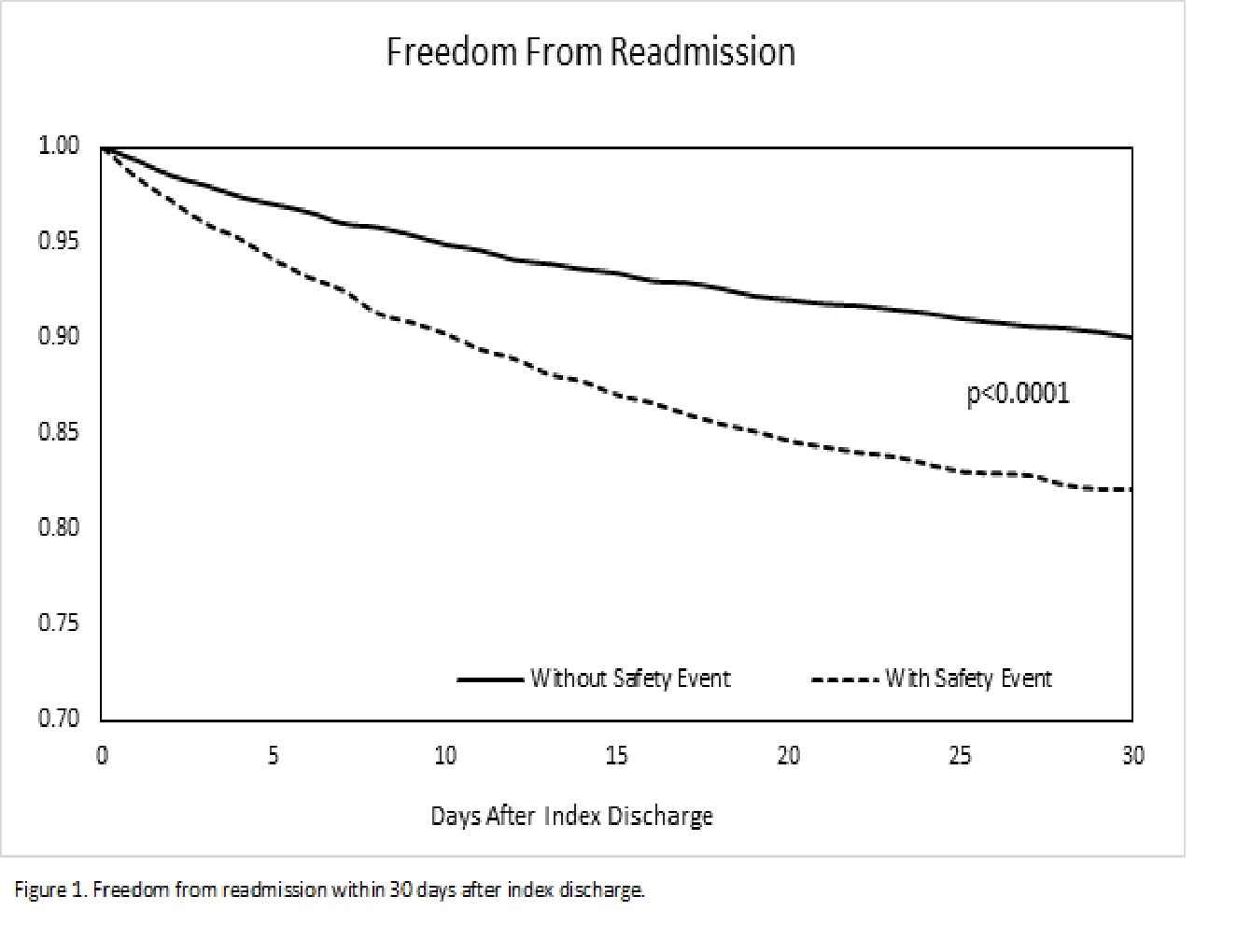
Back to 2018 Program



