
Evaluation of a novel up-and-over transfemoral approach for endovascular repair using iliac branch endoprosthesis in patients with prior bifurcated endografts
Emanuel R. Tenorio, MD, PhD1, Gustavo S. Oderich, MD1, Giuliano A. Sandri, MD1, David Dawson, MD2, Manju Kalra, MD1, Randall R. DeMartino, MD1, Jill K. Johnstone, MD1, Fahad Shuja, MD1.
1Mayo Clinic, Rochester, MN, USA, 2University Of California Davis, Davis, CA, USA.
Objective: Type IB endoleak in patients with bifurcated endografts may be treated by distal iliac branch endoprosthesis (IBE) extension using brachial access for internal iliac artery (IIA) stenting. The aim of this study is to describe a novel "up-and-over" transfemoral technique in patients with prior bifurcated endografts and to compare outcomes with a standard IBE technique for de novo aneurysms.
Methods: We reviewed the clinical data of patients treated for aortoiliac aneurysms using Gore IBE (Flagstaff, AZ) between 2014-2017. A standard technique was indicated for de novo aneurysms and "up-and-over" technique for type IB endoleaks in flared limbs of bifurcated endografts. The "up-and-over" technique used bilateral transfemoral access with a 12-Fr flexible sheath advanced up-and-over the flow divider of the bifurcated endograft for IIA stenting (Figure). End-points were technical success, mortality, major adverse events (MAEs), IIA patency and branch instability (any endoleak, stenosis or occlusion or reintervention) and reintervention.
Results: There were 44 patients (43 male, 73.5±7.8 years old) treated by IBEs (5 bilateral) using standard (n=30) or "up-and-over" technique (n=14). Procedure time, contrast volume and radiation dose averaged 160±99min, 139±51ml and 1086±1168mGy, with no difference between techniques. Technical success was achieved in all patients, but one patient treated by "up and over" technique required brachial access to complete the repair. Ten patients (8 standard, 2 "up-and-over") had extension of the IIA stent into a posterior branch. There was no mortality. Three patients (7%) had MAEs (all EBL>1000ml). Median follow-up was 6 months (interquartile range, 4-9 months). There were 2 IIA stent occlusions, 1 IIA type IB endoleak and 2 reinterventions, all after standard technique. At 1-year, patients treated by standard or "up-and-over" technique had similar primary (91±6% vs. 100%, P=0.34) and secondary patency (95±5% vs. 100%, P=.5), freedom from branch instability (87±2% vs. 100%, P=.26) and freedom from reintervention (92±5% vs. 100%, P=.38).
Conclusions: Endovascular repair using IBEs was associated with high technical success, no mortality and low rate of complications using standard or "up-and-over" technique. Distal IBE extension using "up-and-over" technique is a suitable alternative to brachial access in patients with type IB endoleaks after bifurcated endografts. 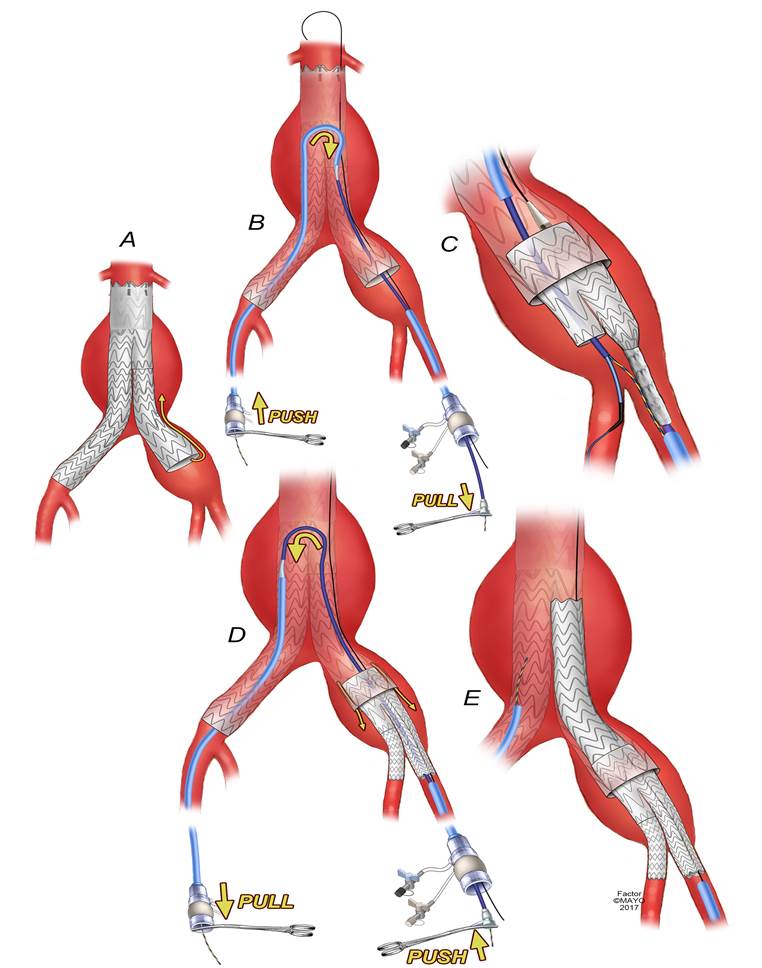
Back to 2018 Program



