
Debranching for Endoleak following Type IA endoleak after APTUS stapler
Jonathan R. Thompson, MD, Matthew Corriere, MD.
University of Michigan, Ann Arbor, MI, USA.
OBJECTIVES: Endovascular anchoring systems, such as endovascular screws or staple fixation devices, have gained increasing popularity for use in treating type I endoleaks. We present a case where debranching and TEVAR were required after attempted treatment with proximal extensions and over 20 fixation devices placed through 3 stent-graft layers failed to resolve the endoleak and eliminated conversion to open repair as a treatment option.
METHODS: A 68-year-old male had a 5.5 cm AAA repaired with EVAR. A routine surveillance CTA performed one year later was negative for sac enlargement or endoleak. He presented with acute abdominal pain one year later, and repeat CTA demonstrated a new type IA endoleak with sac enlargement. Two proximal cuffs, one Palmaz stent, and 28 endo-anchors were placed which failed to resolve the endoleak prior to transfer to our center. There was concern that explantation with conversion to open repair would be technically difficult and potentially unsafe due to the multiple layers of endografts and stents, suprarenal fixation, and endo-anchors. A lumbar drain was placed prior to proceeding with visceral debranching of the abdominal aorta (retrograde bypass from left common iliac artery to the celiac artery, superior mesenteric artery, left main renal artery, left accessory renal artery, and right renal artery) and coverage of the descending thoracic aorta and visceral segment of the abdominal aorta. The distal landing zone was inside the previously placed endograft and extensions.
RESULTS: The patient’s abdominal pain resolved, and postoperative CTA demonstrated endoleak resolution without further aneurysm growth.
CONCLUSIONS: Endo-anchor fixation permits endovascular treatment in the setting of challenging anatomy, but use of multiple fixation devices in combination with multilayered grafts/stents may compromise the safety of conversion to open repair when type IA endoleak treatment is technically unsuccessful. Visceral debranching can be used to treat unresolved type IA endoleak when aggressive use of endo-anchors is unsuccessful and eliminates standard open conversion as an option. 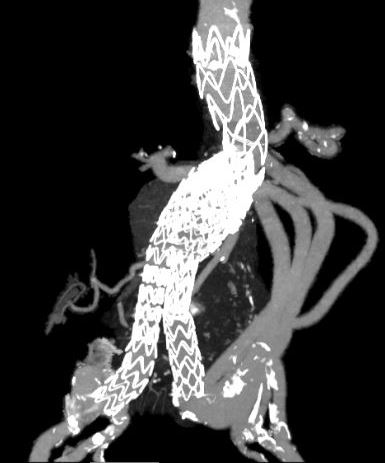
Back to 2018 ePosters



