
Central Venous Recannulation and AV Access Formation in Patients with Central Venous Occlusion
Kira N. Long, MD, Diane Fodor, APN, Rakesh Navuluri, MD, Robert Steppacher, MD, Trissa Babrowski, MD.
University of Chicago, Chicago, IL, USA.
OBJECTIVE - Prevalence of symptomatic central venous obstruction (CVO) is unknown, however it does present a challenge to the more than 400,000 patients undergoing hemodialysis (HD) in the United States. We present two cases of central venous recannulation followed by arteriovenous fistula (AVF) or arteriovenous graft (AVG) formation as a viable option for ESRD patients with CVO, and an alternative to HeRO Graft placement or lower extremity access.
METHODS - Case 1- A 42-year-old man with multiple failed upper extremity accesses underwent radiofrequency recannulation of his SVC with a Baylis Medical PowerWire. Three days later, he was taken to the OR for AVG placement. He had residual stenosis of his right axillary vein, so a Gore Hybrid Vascular Graft was placed with immediate improvement in outflow.
Case 2- A 33-year-old woman with known CVO and a history of multiple failed kidney transplants as well as failed upper and lower extremity AV accesses presented for evaluation for permanent HD access. She underwent a venogram with recannulation of her right brachiocephalic vein and SVC via balloon angioplasty and stent placement. One month later she underwent the first stage of a brachial-basilic AVF creation.
RESULTS - Case 1- One- and two-month post-operative AVG duplexes revealed flow volumes of 1379mL/min to 1663mL/min increasing to 2208mL/min to 4622mL/min, respectively. He has required three AVG declots and CVO angioplasties since that time, however his AVG remains usable.
Case 2- Duplex of the AVF six weeks post-op revealed appropriate maturation with no recurrent CVO. Flow volumes ranged from 248mL/min to 441mL/min with outflow vein diameters ranging from 4.2mm to 5.9mm. At that point she was ready for the second stage transposition of the basilic vein.
CONCLUSIONS - Central venous recannulation followed by native AVF or AVG provides a viable option for HD access in patients with poor venous outflow. This option allows for eventual removal of CVCs and access for HD using an upper extremity conduit. 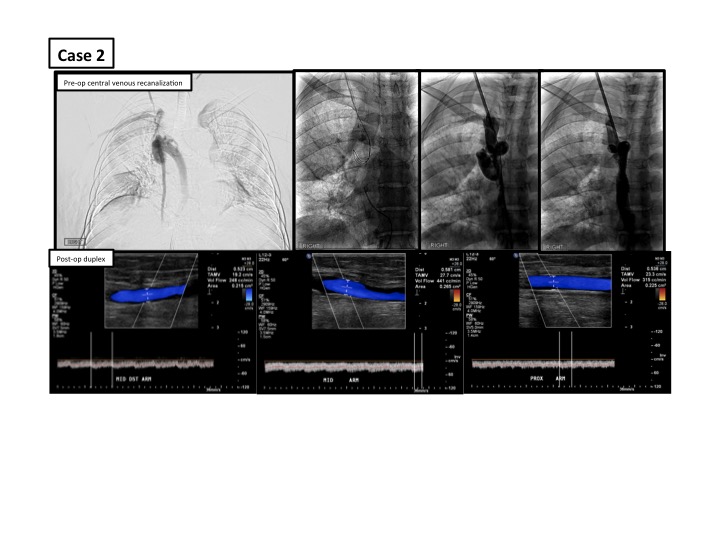
Back to 2018 ePosters



