
Urgent carotid intervention in patients with minor to moderate strokes (NIHSS ≤ 10) performed after 48 hours results in greater functional independence at discharge
Esther Mihindu, DO, Alaa Mohammed, Bethany Jennings, Mustafa Alhasan, MD, James Milburn, MD, Taylor Smith, MD, Clayton Brinster, MD, WC Sternbergh III, MD, Hernan Bazan, MD.
Ochsner Clinic Foundation, New Orleans, LA, USA.
Objective:
Increasing evidence suggests that urgent carotid intervention after a non-disabling stroke is safe, however functional outcome has not been quantified for various degrees of stroke. We aimed to determine whether increased presenting stroke severity is associated with poor functional outcomes in patients undergoing urgent carotid endarterectomy (CEA) or carotid artery stenting (CAS).
Methods
We reviewed all urgent carotid interventions from January 2013 thru April 2017 at a single, tertiary referral center. Preoperative variables analyzed included admit stroke severity, calculated by National Institute of Health Stroke Scale (NIHSS). Primary endpoint was patient functional independence at discharge, quantified by modified Rankin Scale (mRS; ≤2 functional independent, >2 dependent).
Results
A total of 120 urgent carotid interventions [CEA (n=96), CAS (n=22), one CEA with middle cerebral artery aspiration thrombectomy and one carotid embolectomy] were performed. The cohort, when divided into patients with an admit NIHSS ≤ 10 and >10, demonstrated correlation when compared to mRS (p=0.0029). Patients presenting with large strokes, NIHSS >10, were nearly four times more likely to have functional dependence (mRS > 2) at discharge than patients presenting with minor to moderate strokes (NIHSS ≤10, Table).
Time from presentation to CEA/CAS, quantified as days to procedure ≤2 and >2, was also significantly associated with discharge mRS (p=0.0007). Patients undergoing CEA/CAS ≤2 days from presenting symptom were 3.4 times more likely than patients undergoing CEA/CAS >2 days to be discharged with decreased functional dependence, mRS > 2 (OR 3.4; Table). Even when emergent carotid interventions were excluded,
discharge mRS correlated with time to procedure [days 1 – 2 compared to >2 days (p=0.012)]. The odds of having a discharge mRS ≥3 were 3.4 times more likely for patients with procedure performed at 1-2 days compared to >2 days (OR 3.4, Table).
Conclusions
Urgent carotid interventions performed in select patients with minor to moderate strokes (NIHSS ≤ 10) after 48 hours results in functional independence (mRS < 2). By demonstrating a clear correlation between admission NIHSS and interval time to procedure with independent functional outcomes, we aim to clarify clinical decision-making for patients presenting with acutely symptomatic carotid lesions. 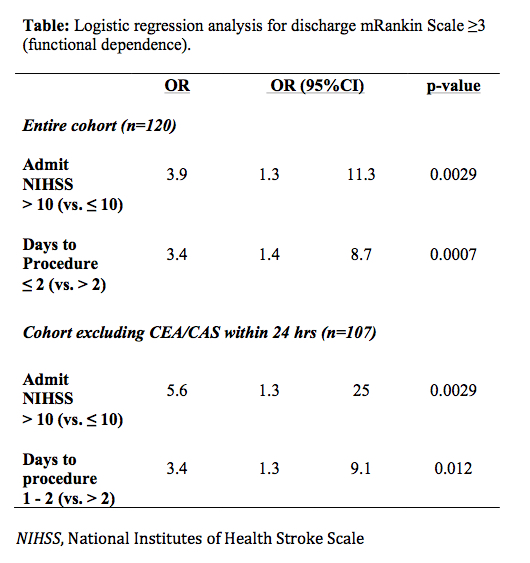
Back to 2018 ePosters



