
Lower Extremity Deep Venous Thrombosis in Renal Transplant: An Unusual Cause of Graft Dysfunction
Ali Khalifeh, MD, J Devin B. Watson, MD, Nandakumar Menon, MD, Michaella Reif, BS, Janet Karanja, BS, Sarah Rosenberger, MS, CRNP, Suzanna Fitzpatrick, MS, CRNP, Rajabrata Sarkar, MD, PhD, Shahab Toursavadkohi, MD.
University of Maryland Medical Center, Baltimore, MD, USA.
Objectives:
Renal transplantation(RT) remains the optimal treatment for end-stage renal disease(ESRD). Graft dysfunction can be a sign of immunological, anatomic or vascular complications. We present a case series of graft dysfunction secondary to ipsilateral lower extremity DVT.
Methods and Results:
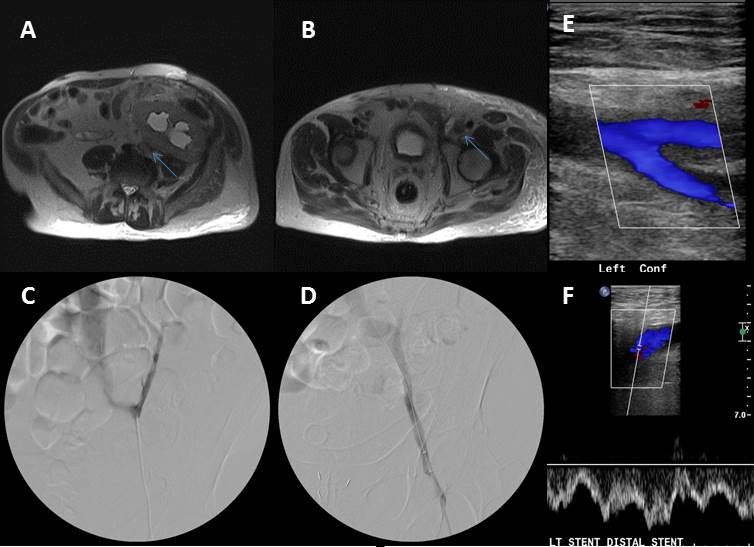
A 70 yo man with ESRD underwent a living unrelated RT with graft placed in left iliac fossa. The patient had immediate graft function and improvement in creatinine clearance(5 to 0.9mg/dL). The patient was evaluated postoperatively for LLE edema with no evidence of DVT. He presented 2months postoperatively with elevated serum creatinine (1.3mg/dL) and persistent LLE edema. A MRA/V of the pelvis demonstrated new hydronephrosis and CFV to EIV thrombosis. The patient was taken to the OR for management. IVUS was used to evaluate extent of thrombus then we proceeded with pharmaco-mechanical thrombolysis of the CFV and EIV via left popliteal access. This was followed by EIV angioplasty and stenting. On 12months follow up , the patient has had resolution of LE edema, and Cr nadir of 0.85mg/dL.
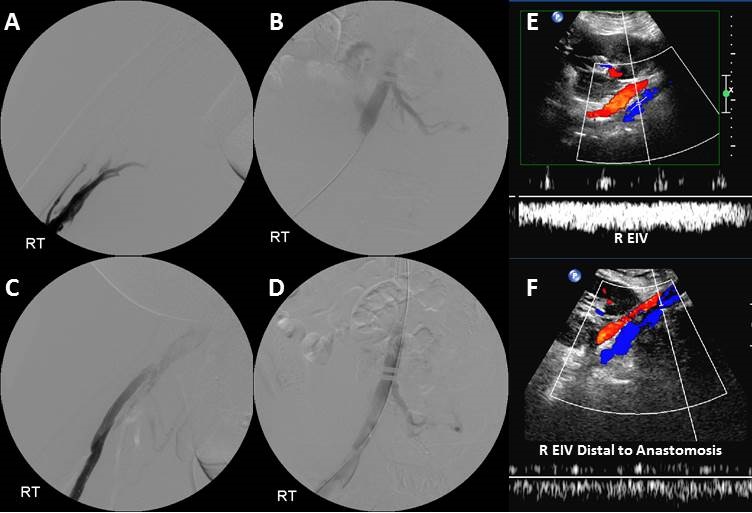
Second case was a 43 yo man with ESRD secondary to type-1 diabetes who initially underwent a simultaneous kidney-pancreas transplant and subsequent living RT for failed renal graft . The new renal allograft was placed in the right iliac fossa. Three-years postoperatively the patient presented to the transplant service with an acute kidney injury (Cr rise 1.3 to 2.85mg/dL). Ultrasound duplex exam demonstrated patent graft vasculature with Right EIV and CFV thrombosis. The patient was taken to the OR where popliteal access was used. IVUS was used to evaluate extent of thrombus which confirmed iliofemoral DVT. The thrombus was cleared using pharmaco-mechanical thrombolysis. The patient Cr returned to 1.3mg/dL and was discharged on oral anticoagulation.
Conclusions:
Venous thrombosis of the ilio-femoral system should be ruled out when evaluating for renal allograft dysfunction. We believe that an acute DVT can sufficiently impede venous outflow leading to acute graft dysfunction. This may be an under-recognized cause of graft dysfunction.
Back to 2018 ePosters



