
Surveillance and Management of Troponin Elevation after Vascular Surgery
Mrinal Shukla, MD, Peter W. Callas, Ph.D, Julie A. Lahiri, MD, Matthew J. Alef, MD, Friederike Keating, MD, David J. Schneider, MD, Andrew C. Stanley, MD, Georg Steinthorsson, MD, Daniel Bertes, MD.
University of Vermont Medical Center, Burlington, VT, USA.
OBJECTIVES: To implement a postoperative troponin surveillance algorithm aimed at intensifying medical management after vascular surgery.
METHODS: We conducted a single-center study of postoperative troponin surveillance after vascular surgery (N=201) at a tertiary care, academic medical center from January to December 2016. Troponin surveillance was performed on postoperative days 1-3 regardless of cardiac symptoms. Patients with troponin I elevation (>.034 ng/mL) were managed with a treatment algorithm which included single or dual antiplatelet (AP) agent, high intensity statin, smoking cessation consultation and outpatient cardiology consultation and stress testing. Patients with troponin elevation ≥1.0 ng/mL received inpatient cardiology consultation. We retrospectively assessed adherence to the protocol with regard to intensification of best medical therapy defined as high dose statin, increase in antiplatelet therapy, and smoking cessation consultation in active smokers.
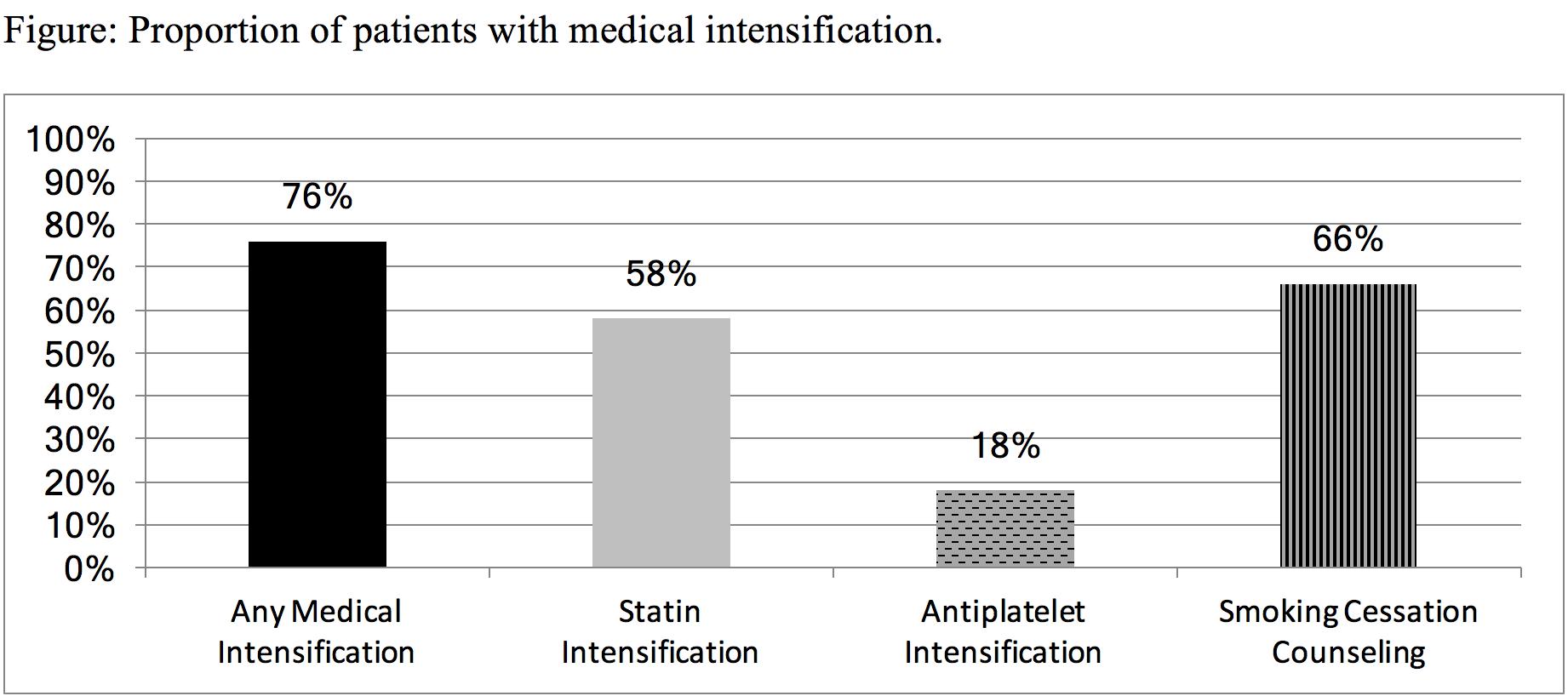
RESULTS: Troponin elevation (34/201) was associated with a symptomatic cardiac event in 8 patients (24%) while 26 (76.5%) had an asymptomatic abnormal troponin on postoperative surveillance. Troponin elevation ≥1.0 ng/mL occurred in 11 asymptomatic patients (5.5%). Any intensification of medical therapy (N=33, one patient excluded due to death) was instituted in 76% of patients; high dose statin therapy (58%), increase in AP therapy (18%) and smoking cessation consultation (66%) of patients (Fig.). Once an elevated troponin level was recognized, 52% of our patients received cardiology consultation with an increased likelihood (100%) in patients with troponin ≥1 ng/mL. Adherence to outpatient stress testing was low at 18%. Intensification of medical therapy was not significantly different between patients with positive troponin >.034-1.0 (N=23) vs. ≥1.0 ng/mL (N=10); statin therapy (P=1.0), antiplatelet (P=0.34), and smoking cessation (P=1.0). Cardiology consultation was more frequent in patients with troponin elevation ≥1.0 ng/mL compared to >.034-1.0 (P < 0.001).
CONCLUSIONS: Routine postoperative troponin surveillance protocol results in intensification of medical management of patients with asymptomatic troponin elevation. Further study is needed to determine if this approach reduces long term cardiovascular morbidity and mortality.
Back to 2018 ePosters



