
Billowing of Endologix AFX Abdominal Aortic Aneurysm Device as a Precursor for the Rupture of an Abdominal Aortic Aneurysm
Heepeel Chang, MD, Neal C. Hadro, MD, Marc A. Norris, MD, Sang Won Rhee, MD, Marvin E. Morris, MD.
Baystate Medical Center, University of Massachusetts Medical School, Springfield, MA, USA.
OBJECTIVE:
Despite a recent publication indicating billowing (aneurysmal degeneration of the outer fabric material manifesting as a bulging sac of contained contrast due to weakening of the fabric material between the metal struts) as a benign finding, we report a case of billowing with the Endologix AFX® graft that resulted in aneurysmal rupture. AFX® consists of an inner metallic endoskeleton with multiple metallic struts covered by a polytetrafluoroethylene graft fabric. As the outer cover is anchored to the endoskeleton with polypropylene sutures only at the proximal and distal ends, AFX® graft can allow flow of blood or contrast beyond the border of the metallic endoskeleton without evidence of endoleak or rupture.
METHODS:
Electronic medical records were reviewed to retrieve images, operative details and findings at presentation.
RESULTS:
An asymptomatic 90-year-old-male with an infrarenal AAA underwent an endovascular repair with the AFX® device according to current instruction for use, with 45mm overlap of main body and proximal aortic cuff. The aneurysm neck diameter, length and angle were 27mm, 19mm and 56ş, respectively. After 24 months, he presented to the ED with back pain. Initial computer tomography angiography (CTA) showed stable AAA with contrast accumulation in-between the metal struts circumferentially, representing type I billowing. After 3 days, due to persistent pain, he underwent a repeat CTA, which demonstrated rapidly expanding AAA sac up to 8.1x6.9 cm with active extravasation. He underwent emergent balloon occlusion of the aorta, followed by successful endovascular repair with aorto-uni-iliac device (Cook Medical) stent grafting and femoral-to-femoral bypass.
CONCLUSIONS:
Billowing represents a unique manifestation of the AFX® AAA stent-graft. Despite initial absence of evidence of endoleak or sac enlargement in this patient, our findings suggest that this phenomenon may mandate an urgent repair of the AAA secondary to the continued pressurization of the AAA sac. Future research should be aimed at determining if further modifications of the AFX® device are required to mitigate this potentially fatal complication.
FIGURES:
A. Billowing (arrow) of AFX-stentgraft without evidence of endoleak or rupture.
B. Expanding AAA with aortic rupture (arrow).
C. 3D rendering in-situ reconstructed from CTA demonstrating aortic rupture with exsanguination (arrow). 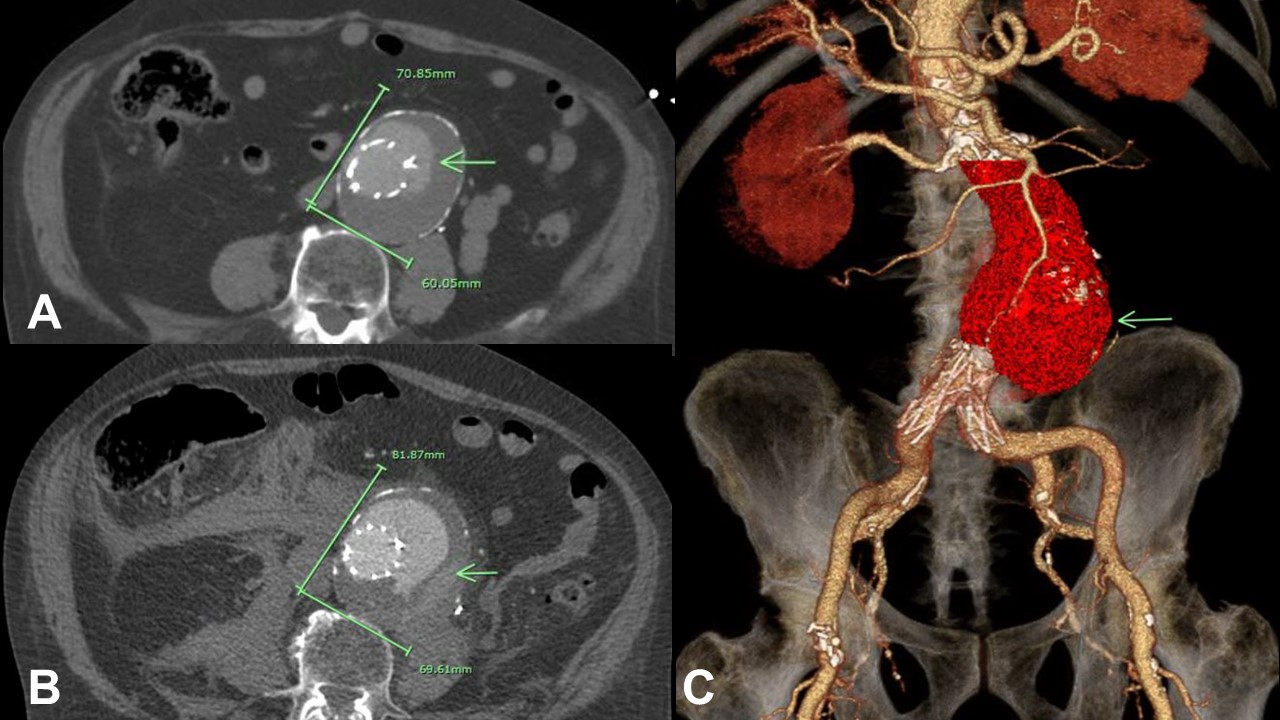
Back to 2018 ePosters



